
12% of Physicians Remain Independent. Now They're Writing the Checks.
While $14.2 billion in healthcare venture capital flowed last year, almost none of it reached independent physicians. PhyCap Fund inverts the model.

Physicians and clinicians generate the revenue.
Physicians and clinicians carry the clinical risk.
Someone else owns the equity.
IN TODAY’S ARTICLE:
Why were the capital markets that built your competitors designed to exclude independent physicians
The $14.2 billion flowing into healthcare technology and who’s on the cap tables
How the PhyCap Fund is structured to put physicians on the equity side for the first time
How to get in at $50K minimum before the fund closes
Glossary at the bottom of today’s article.
THE CAPITAL EXCLUSION
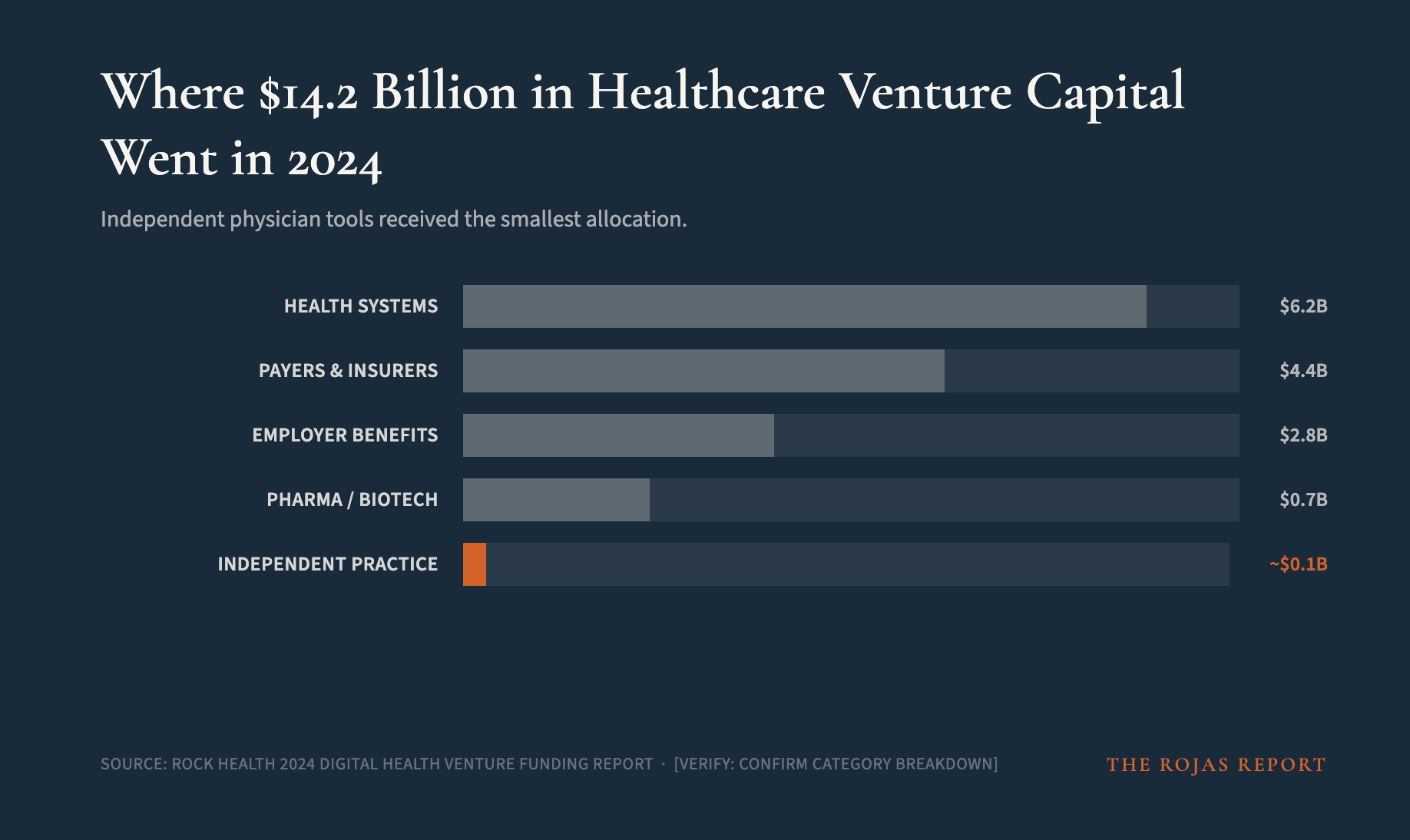
$14.2 billion in healthcare venture capital was deployed last year.
Almost none of it reached independent physicians.
The technology that funding built was designed for health systems: revenue cycle platforms, clinical decision tools, and workflow management systems. It integrates with the health system infrastructure. It scales inside hospital contracts. It makes hospital operations more efficient.
That is not neutral. That is strategic.
Every dollar of healthcare technology capital that flows into the hospital orbit makes hospital-affiliated practices more efficient and independent practices comparatively less efficient. The financing gap is not a market failure. It is the market working exactly as designed.
The healthcare cartel counts on you not paying attention.
100,000+ physicians refuse to comply. Join them.
THE 12% PROBLEM
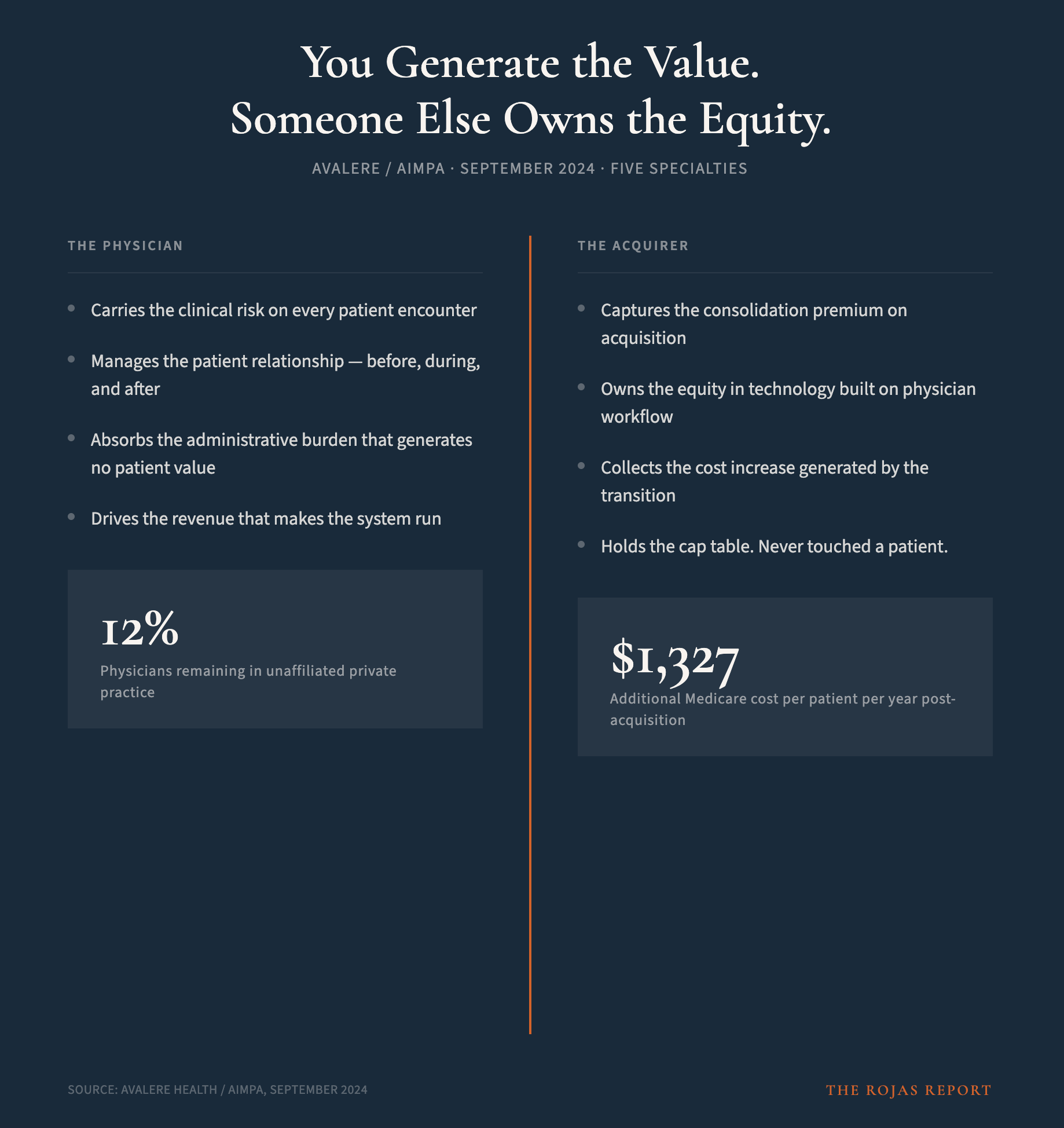
Avalere studied physician practice affiliation models across five specialties in September 2024.
12% of physicians remain in unaffiliated private practice.
When physicians transitioned to hospital employment, Medicare costs increased $1,327 per patient per year. That value did not disappear. It moved. It moved to the hospital system balance sheet — and to the equity held by the institutions and investors who financed the consolidation.
Physicians generated that value. Physicians bore the patient relationships, the clinical risk, and the administrative burden that made consolidation possible. Someone else owns the upside.
For thirty years, that asymmetry was treated as inevitable. It is not inevitable. It is a financing gap.
THE FUND
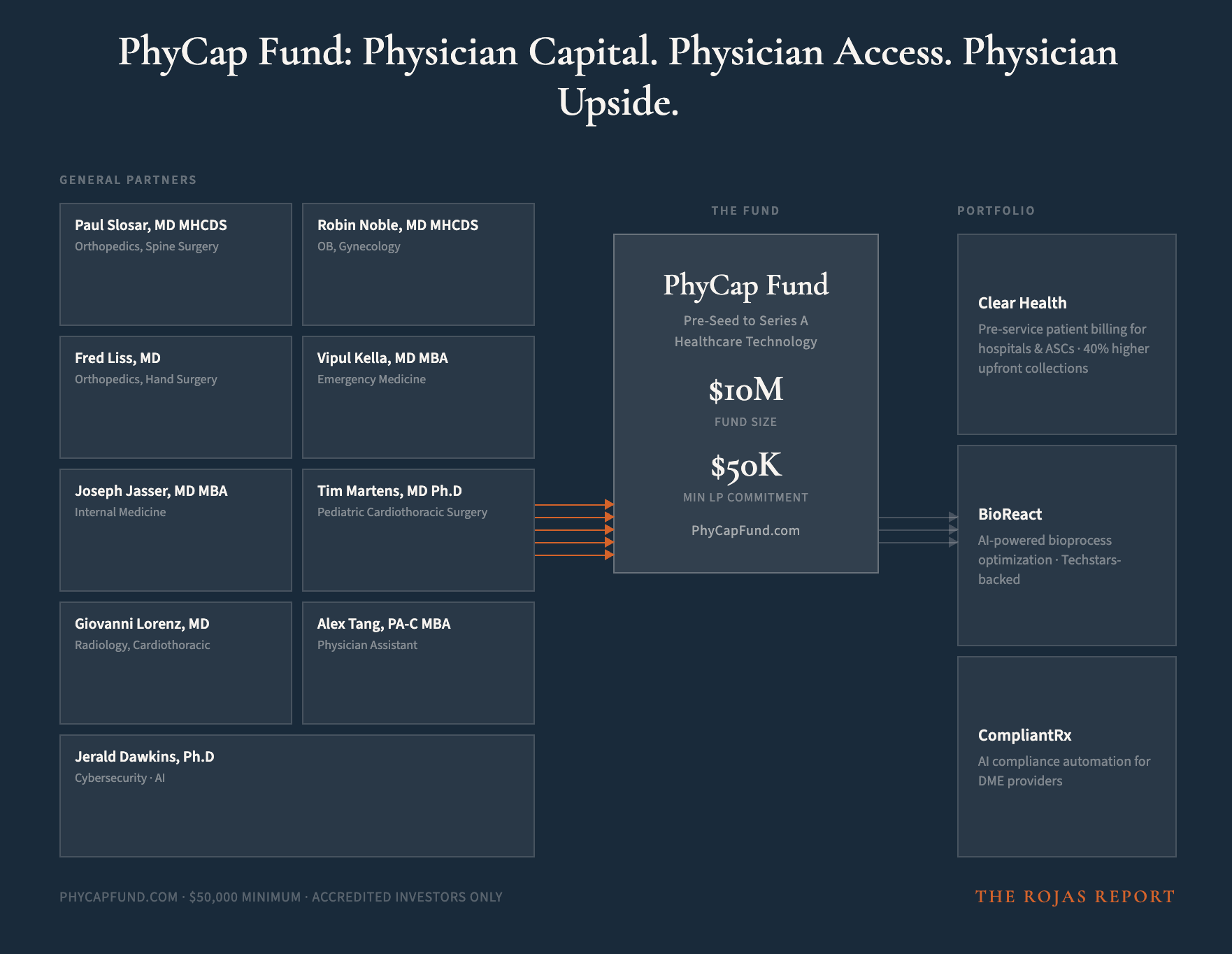
PhyCap Fund is a $10 million early-stage venture fund investing Pre-Seed through Series A in healthcare technology companies.
The focus is narrow: companies that reduce the structural disadvantages that make independent practice harder than it has to be. Administrative burden. Workflow dysfunction. Billing and compliance friction consumes clinical time and generates no patient value.
The people who built this fund are not analysts. They are practicing physicians and clinicians who live inside the problems the portfolio companies are solving.
The PhyCap General Partners:
Paul Slosar, MD MHCDS — Orthopedics, Spine Surgery
Robin Noble, MD, MHCDS — OB, Gynecology
Fred Liss, MD — Orthopedics, Hand Surgery
Vipul Kella, MD, MBA — Emergency Medicine
Joseph Jasser, MD, MBA — Internal Medicine
Tim Martens, MD Ph.D — Pediatric Cardiothoracic Surgery
Giovanni Lorenz, MD — Radiology, Cardiothoracic
Alex Tang, PA-C, MBA — Physician Assistant
8 GPs. Seven specialties. Every one of them has sat across the table from a patient while the administrative weight of a broken system piled up behind them.
The current portfolio:
Clear Health — pre-service patient billing platform for hospitals and ASCs, consolidating all provider and insurance charges into one bill and driving 40% higher upfront collections before the patient arrives.
BioReact — AI-powered bioprocess optimization platform, running up to 10,000 in-silico simulations to identify optimal conditions before a single experiment runs. Techstars-backed.
CompliantRx — AI compliance automation for DME providers, catching documentation gaps before claims are denied and reducing audit risk.
PhyCap selected each company because it attacks a problem this publication has spent months documenting. The thesis is not abstract. The documentation is in the archive.
You can learn how the system works.
Or you can keep being surprised when it works against you.
Subscribe
WHY PHYSICIAN GPS ARE DIFFERENT
The Silicon Valley venture capital brings a network of engineers, operators, and institutional relationships.
PhyCap physicians bring something that cannot be purchased: clinical credibility and real-world market access inside the practices that will adopt or reject a product.
When a PhyCap portfolio company needs to validate a workflow tool, it does not hire a consulting firm to simulate physician behavior.
It has practicing physicians and clinicians already inside the fund who can test, critique, and champion from day one. That shortens the feedback loop. It eliminates credentialing delays that can kill otherwise viable products before they reach scale.
A pediatric cardiothoracic surgeon.
Orthopedic surgeons.
An emergency physician.
An OB-GYN. A hand surgeon.
A radiologist.
A PA.
An internist.
That is ’t a board of advisors assembled for optics.
That is a clinical and technical intelligence network embedded in the fund structure.
THE TERMS
Fund size: $10 million.
Minimum LP commitment: $50,000.
Accredited investor status required.
Investment stage: Pre-Seed to Series A.
Sector focus: Healthcare technology reducing barriers to independent practice.
The conversation starts at PhyCapFund.com.
No one is coming to save independent medicine.
So we’re saving each other. 100,000+ physicians. One signal.
Subscribe
THE CLOSING ARGUMENT
The consolidation playbook has been running for three decades.
It has been financed by capital markets. It has been protected by policy. It has been accelerated by technology built specifically for the acquirer.
The architects of that playbook counted on independent physicians being too busy, too isolated, and too excluded from capital to build a counterweight.
PhyCap Fund is the counterweight.
The physicians who read this publication have already accepted the thesis. The fund does not need to educate them on the opportunity. They documented it.
If you want to invest in the infrastructure that supports independent practice rather than watch someone else accumulate the equity your work generates, the conversation starts at PhyCapFund.com.
-Rojas out.
GLOSSARY
LP (Limited Partner): An investor in a venture fund. LPs provide capital; the General Partners make investment decisions. LPs receive returns proportional to their investment when portfolio companies exit.
GP (General Partner): The managing partners of a venture fund who make investment decisions, source deals, and work actively with portfolio companies. PhyCap’s GPs are practicing physicians and clinicians, not professional investors.
Pre-Seed / Series A: Funding stages for early-stage companies. Pre-Seed is the earliest institutional capital, often before a product has significant revenue. Series A is the first major institutional round, typically after a product has demonstrated market traction.
Accredited Investor: An individual or entity that meets SEC income or net worth thresholds, qualifying them to invest in private securities offerings not registered with the SEC.
Unaffiliated Private Practice: A physician practice with no ownership or employment relationship with a hospital system, health system, or corporate entity. The 12% figure from Avalere (2024) refers to this category.
Cap Table: A record of who owns equity in a company and in what proportion. “Being on the cap table” means holding an ownership stake in a company, not merely providing labor or services.
SOURCES
Avalere Health / AIMPA. Medicare Service Use and Expenditures Across Physician Practice Affiliation Models. September 2024.
Rock Health. 2024 Digital Health Venture Funding Report. Rock Health, 2024.
If the system is designed to exclude independent physicians from capital, it suggests the real bottleneck isn’t just access—but the financial infrastructure itself.
Curious whether enabling ownership requires not just new funds, but new rails entirely.