
$15.6 Million Per ASC. Ascension Just Priced Every Physician-Owned Center in America.
The next 12 months will sort the owners who read the signal from the owners who only read the offer.

Becker’s framed it as a race.
The chains framed it as consolidation.
Wall Street framed it as a roll-up.Every framing has the same payoff.
Physicians sell.
PE compounds.There is a structure where physicians compound.
IN TODAY’S ARTICLE:
Why selling at 12x EBITDA is losing, not winning.
What PE is actually buying. And why physicians keep mispricing it.
The three captives: casualty (with med mal), property (the ASC itself), and health benefits.
The Up-C endgame: liquidity without governance surrender.
Glossary at the bottom of today’s article.
THE FRAMING IS THE TRAP
Becker’s calls it a land grab. The trade press counts doors. USPI sits at 533 centers. SCA sits above 370. AmSurg, combined with Ascension, is above 300 and adding. HCA holds more than 150. Surgery Partners owns 157 after rejecting Bain’s $3.2 billion offer. Tenet has allocated $250 million a year to keep buying.
Independents still own roughly 70 percent of the market.
There is no race.
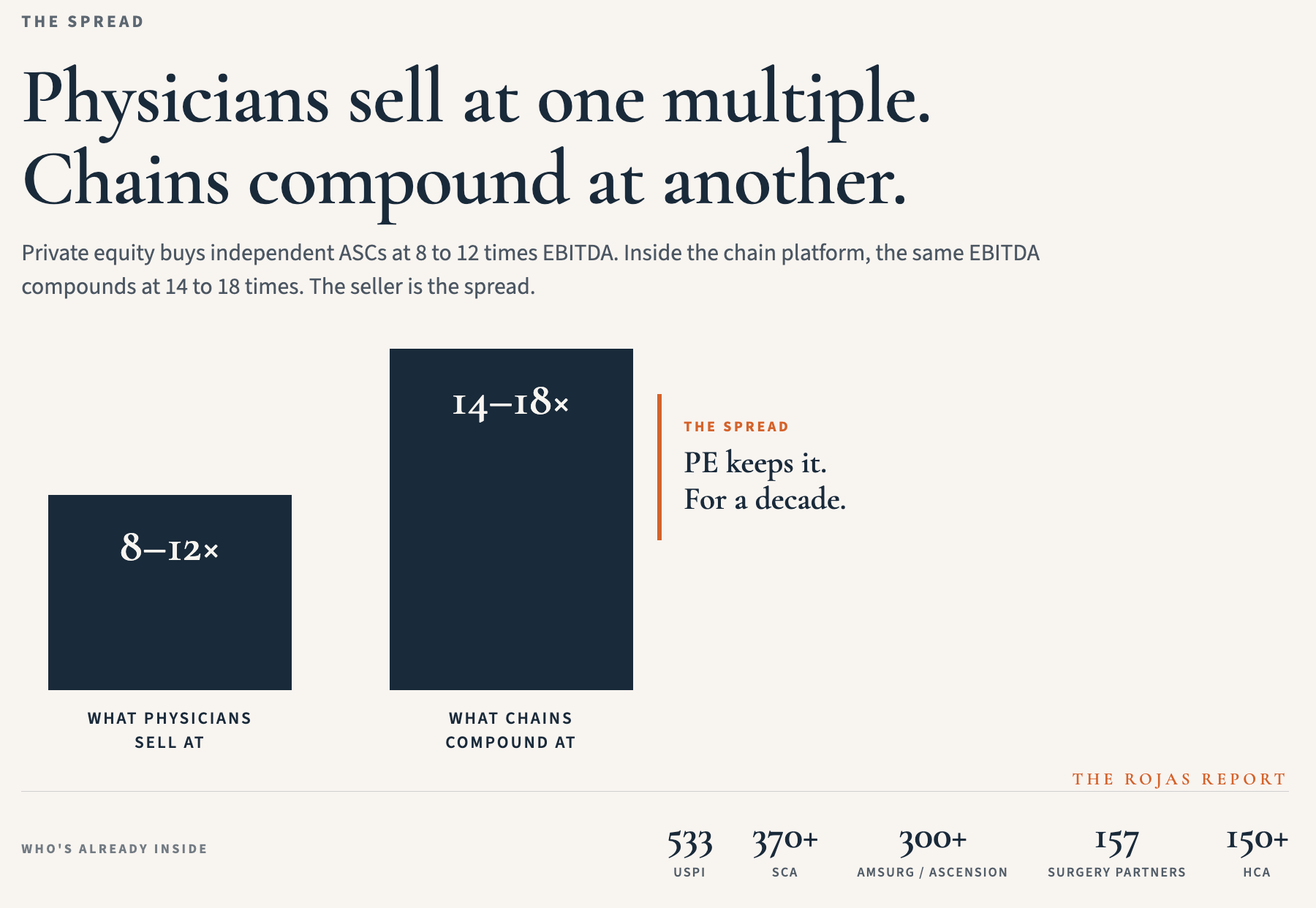
Private equity pays 8 to 12 times EBITDA to bring centers onto their platforms.
Once inside, the same EBITDA compounds at 14-18 times.
Physicians sell at a lower multiple.
The chain keeps the higher returns for years.
That is not winning.
That is forfeiting the compounding before it starts.
WHAT PRIVATE EQUITY IS ACTUALLY BUYING
The building is not the asset. The procedure mix is not the asset. The asset is the long tail underneath: the float on workers’ comp premiums, the float on medical malpractice premiums, the float on self-funded health benefits at an aggregated scale, the rebates on implants that currently route through group purchasing organizations as fees, and the recurring procedure volume booked against fixed real estate.
PE understands this. That is why they pay. The center collects what the payor contract permits. The captive structure beneath the center compounds quietly remains for 30 years. The center is the entry point. The captive is the prize.
Physicians keep selling the entry point and forfeiting the prize.
THE INVERSION
The third structure is built on the inversion of the PE trade.
Private equity offers infrastructure parity in exchange for ownership. The third structure offers infrastructure parity in exchange for participation. The center stays physician-owned. The captive economics route for physicians, rather than leaking to Hartford or Travelers. The float compounds for the people doing the cutting, not for the people writing the check.
That is the entire pitch.
Everything below this line is the architecture that makes it operational.
ANESTHESIA IS THE WEDGE
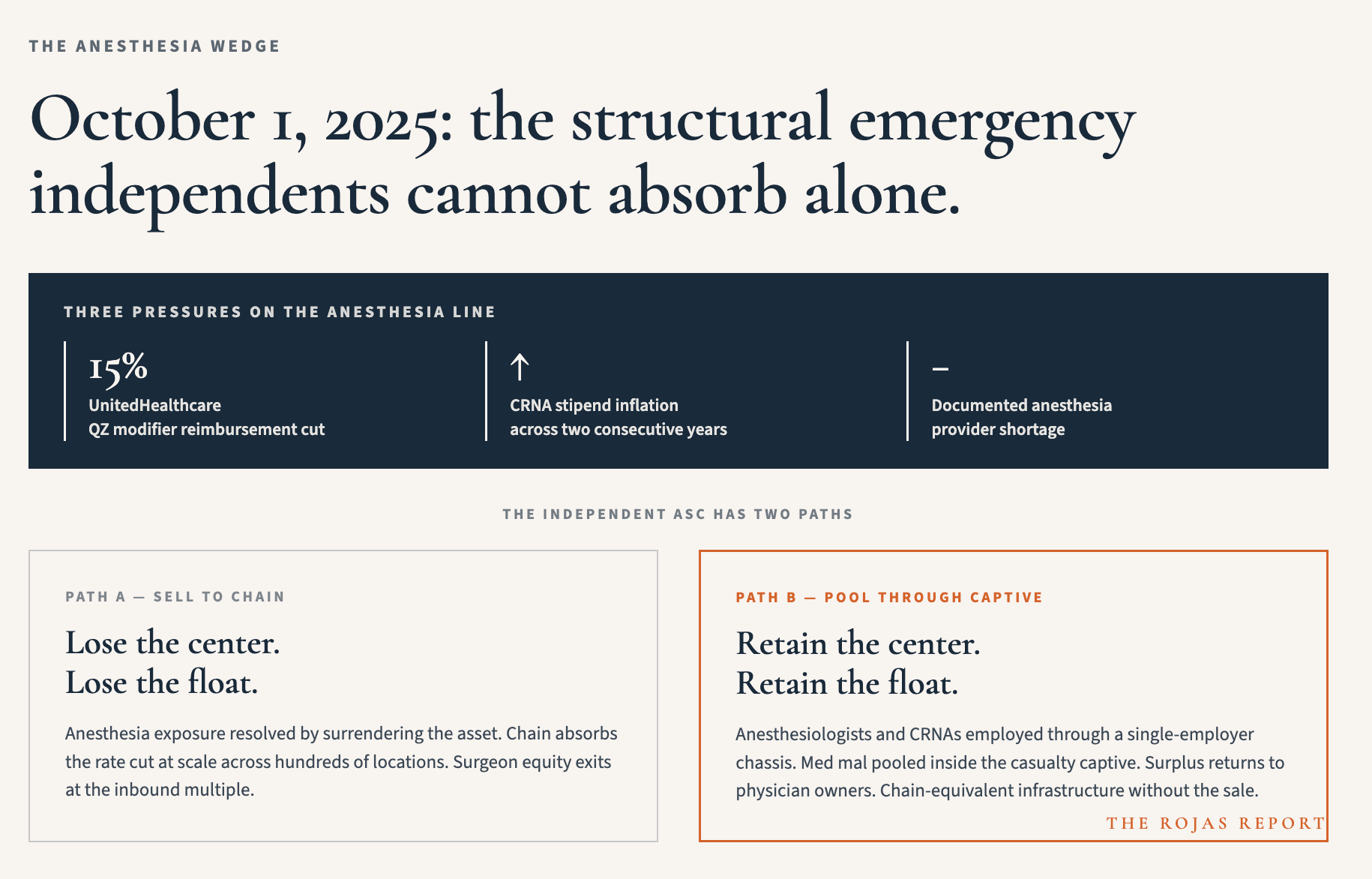
On October 1, UnitedHealthcare cut CRNA reimbursement by 15 percent when billed with the QZ modifier. That cut sits atop two years of stipend inflation and a documented anesthesia shortage. For an independent ASC, this is a structural emergency. For USPI and SCA, it is a marginal annoyance absorbed across 500-plus locations and a national staffing chassis.
A pooled anesthesia structure fixes this differently than a chain acquisition does. Anesthesiologists and CRNAs employed through a single-employer chassis with coordinated benefits and pooled medical malpractice coverage routed through a physician-owned captive. The independent ASC accesses a chain-equivalent anesthesia infrastructure without selling the building.
USPI and SCA cannot match this defensively. They need to extract margin from the anesthesia line because their LPs require it. The captive needs to retain margin because the surplus belongs to the surgeons.
That is the asymmetry. The chain is structurally constrained to bleed anesthesia. The captive is structurally constrained to protect it.
Private equity buys ASCs because they understand what the asset actually is.
Most physicians selling them don’t.
The Rojas Report explains the language difference that makes the trade obvious. 100,000 physicians and healthcare operators read it before the press release.
Subscribe.
