
$486 Million in Lobbying. Six Straight Years of Reimbursement Cuts. What Did They Buy?
The AMA is the 4th largest health sector lobbyist in America. Independent medicine collapsed on their watch. Coincidence or strategy?

$486 million.
That’s how much the AMA has spent on lobbying since 1998. They’re the 4th-largest health-sector lobbyist in America. Top 20 across all industries.
So where did the money go?
Not to protect physician reimbursement. That dropped six years straight. Not to preserve independent practice. That collapsed from 60% to 42%. Not to reduce administrative burden. That’s still increasing.
$486 million.
And physicians lost on every front that matters.
This is the story of what the AMA actually lobbies for.
IN TODAY’S ARTICLE:
The $486 million question: what does the AMA actually lobby for?
The exposed record: six years of Medicare cuts, zero effective resistance
The scope creep silence: 80+ bills blocked in 2024, but not by physician advocates
Why the AMA’s incentives don’t align with independent physicians
Glossary at the bottom of today’s article.
THE EXPOSED RECORD
Medicare Reimbursement
2020: Cut
2021: Cut
2022: Cut
2023: Cut
2024: Cut
2025: Cut
Six straight years.
The AMA lobbied every single year.
Reimbursement dropped every single year.
The 2025 Medicare Physician Fee Schedule cut reimbursement again. The AMA issued press releases. They sent letters. They testified.
The cuts passed anyway.
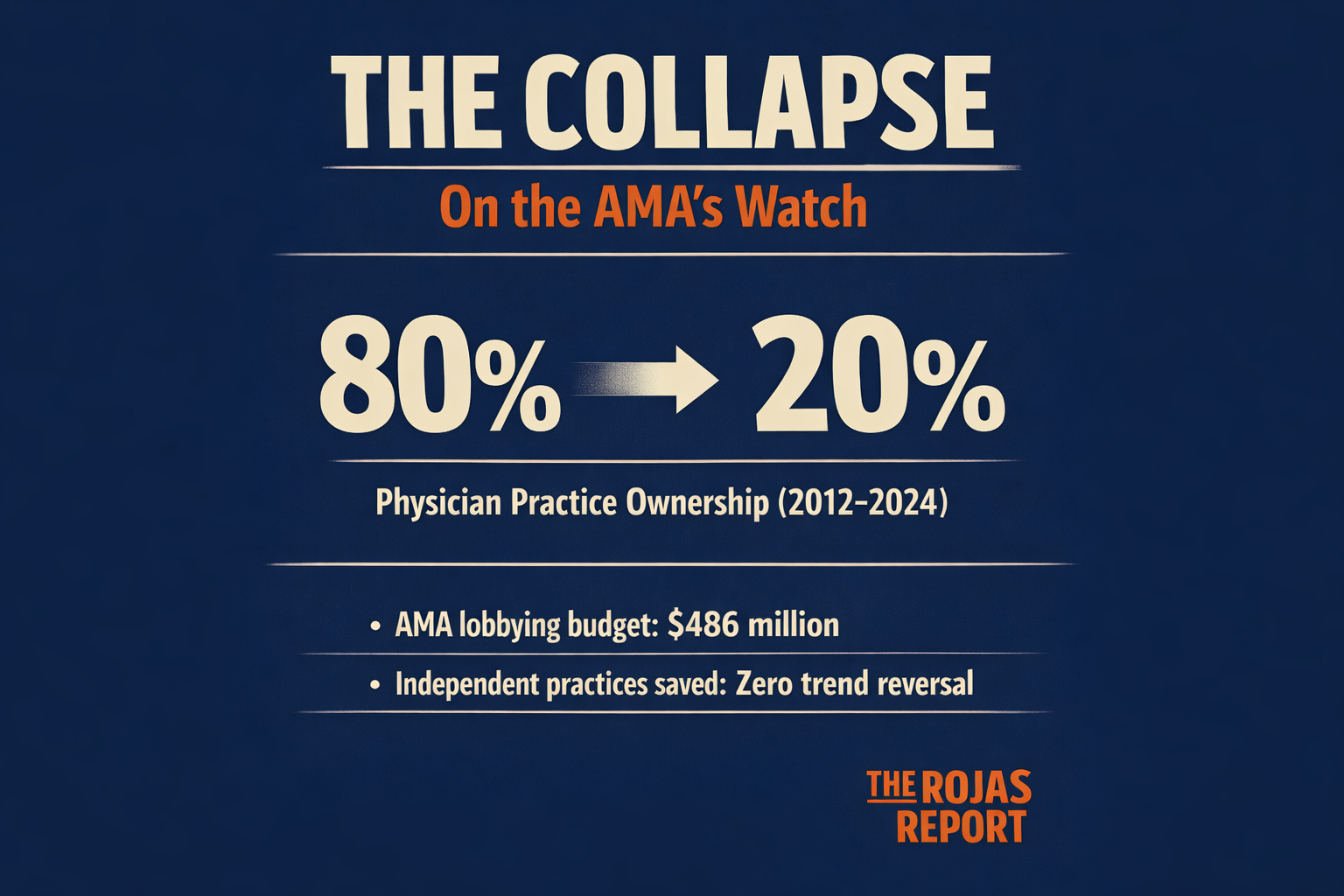
Physician Practice Ownership
2010: 80% of physicians owned their practice, and by 2025, less than 20% of physicians owned their practice. The collapse of independent medicine happened in plain sight.
The AMA had $486 million to fight it.
They didn’t.
Administrative Burden
Prior authorization requirements: Increasing Documentation demands: Increasing Compliance costs: Increasing. The AMA publishes reports about administrative burden. They host conferences. They issue policy statements.
The burden keeps growing.
WHAT THEY ACTUALLY LOBBY FOR
The AMA’s lobbying priorities are public record. OpenSecrets tracks them. The disclosures are filed.
Here’s what the AMA consistently prioritizes:
CPT Code Protection
The AMA lobbies aggressively to maintain its monopoly on billing codes. Any legislative threat to CPT ownership gets immediate attention.
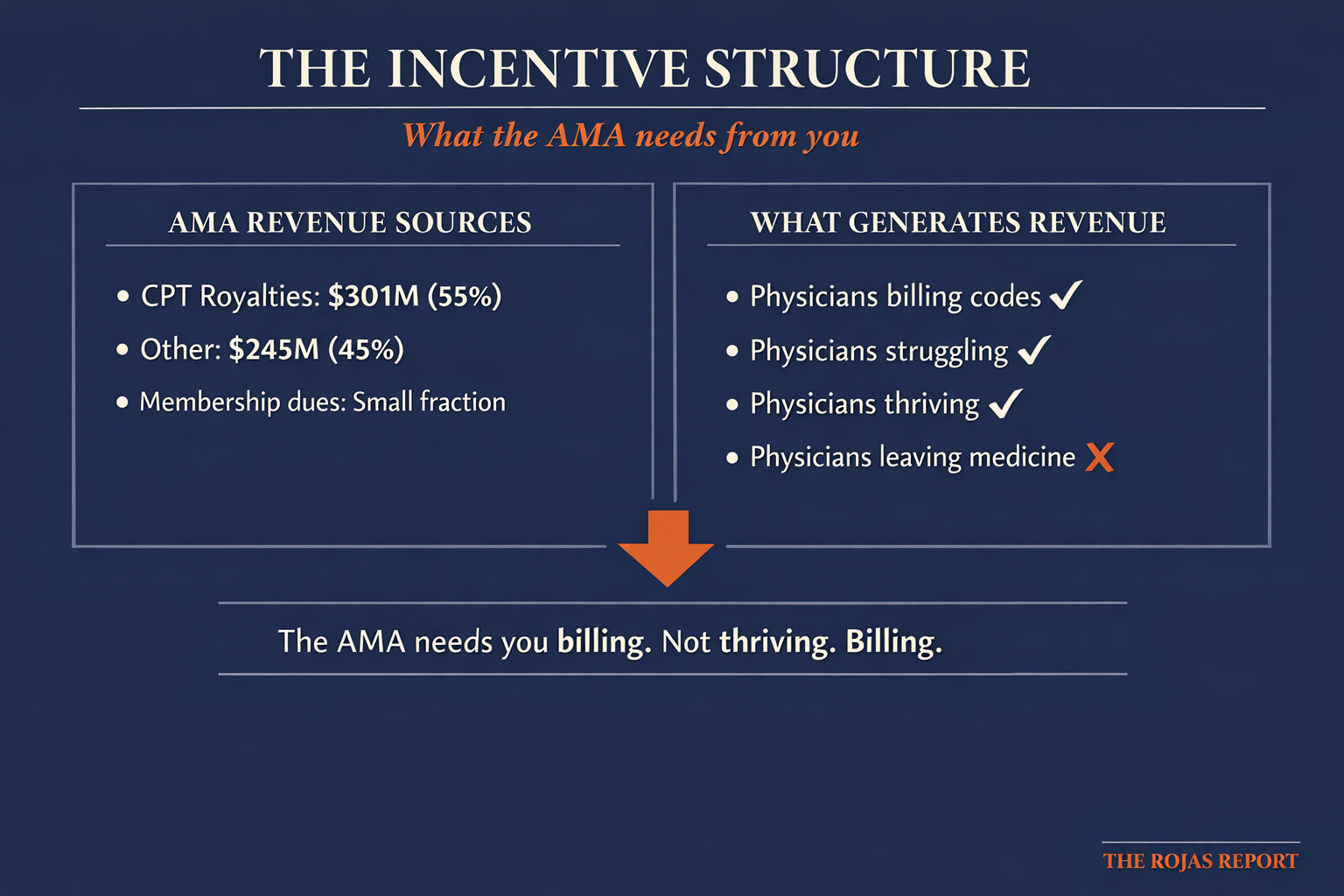
Remember: CPT royalties generate $301 million per year. 55% of AMA revenue.
When your revenue depends on a government-mandated monopoly, you lobby to protect that monopoly.
Scope of Practice
The AMA lobbies against expanding the scope of practice for nurse practitioners, physician assistants, and other non-physician clinicians.
This sounds like physician advocacy. Look closer.
The AMA’s position protects the value of the codes it owns. More billing through physicians means more CPT transactions. More CPT transactions mean more licensing revenue.
Medical School Accreditation
The AMA helps control medical education through the Liaison Committee on Medical Education (LCME). Restricting physician supply has been AMA policy for over a century. Fewer physicians mean higher prices. Higher prices mean higher code values. Higher code values mean more royalty revenue.
This is Part 2 of 5. The receipts continue all week. Everyone in healthcare has an opinion about the AMA. Very few have the 990s. This is where the 990s live.”
Everyone receives: The $486M number, the exposed record (Medicare cuts, ownership collapse, admin burden), what they actually lobby for, CTA
Members receive: The exposed incentive, the scope creep silence, the lobbying paradox explained, and the tomorrow’s teaser. Become a Member.
THE EXPOSED INCENTIVE
Here’s the paradox:
The AMA’s revenue doesn’t depend on physician prosperity. 55% comes from CPT royalties. Physicians pay whether they’re thriving or struggling. Membership dues are a small fraction of revenue. The AMA doesn’t need physicians to join. They need physicians to practice and bill.
A physician working 80 hours a week, drowning in administrative burden, barely breaking even? Still billing CPT codes. Still generating AMA revenue. A physician who sells to a hospital system? Still billing CPT codes. Still generating AMA revenue.
A physician who leaves medicine entirely?
That’s the only scenario where the AMA loses.The AMA’s financial incentive is physician participation, not physician prosperity.
As long as you’re billing, they’re collecting.
THE SCOPE CREEP SILENCE
In 2024, state legislatures introduced over 80 bills expanding the scope of practice for non-physician clinicians.
The AMA’s response: Policy statements. Press releases. Official opposition.
The result: Many bills passed anyway.
Compare this to CPT code protection. When Congress has considered alternatives to CPT, the AMA mobilizes immediately. Lobbyists. Campaign contributions. Direct legislator contact.
The intensity isn’t equal. Protecting CPT revenue gets the full lobbying machine. Protecting the physician's scope of practice gets press releases.
This isn’t incompetence. This is priority revelation.
THE PARADOX EXPLAINED
The AMA isn’t failing at lobbying. They’re succeeding at lobbying for their actual priorities.
Priority 1: Protect CPT monopoly. Status: Protected.
Priority 2: Maintain accreditation control. Status: Maintained.
Priority 3: Preserve organizational revenue. Status: $1.15 billion in net assets.
Physician reimbursement?
Physician independence?
Physician autonomy?
Those aren’t the priorities.
Those are the talking points.
The AMA raised $546 million in 2024. They added to their war chest. They paid executives $11 million.
And physician reimbursement dropped for the sixth straight year.
This isn’t a lobbying failure. This is a lobbying success for an organization whose interests diverged from those of physicians decades ago.
Yesterday, Substack named The Rojas Report #1 in Health Politics.
The cartel’s lobbyists already know what’s in here.
The question is whether you do.
Get your membership here.

THE $486 MILLION QUESTION
What would $486 million in lobbying look like if it actually prioritized physicians?
Sustained campaign against Medicare cuts. Real pressure. Real consequences for legislators who vote against physician reimbursement. Aggressive defense of independent practice. Fighting hospital consolidation. Fighting private equity acquisition.
Actual reduction in administrative burden. Not reports. Not conferences. Legislation. That’s not what happened. $486 million was spent on CPT protection, organizational growth, and executive compensation.
The AMA got exactly what they paid for.
You didn’t.
TOMORROW
COUNT THREE: The Membership Fraud
15% of physicians are AMA members.
The AMA claims to speak for all of American medicine.
How do they justify it?The exposed math.
The proxy game.
The representation they claim but don’t have.
11:30 am Eastern Standard Time.
GLOSSARY
OpenSecrets: A nonpartisan nonprofit that tracks money in politics, including lobbying expenditures. Source for AMA lobbying data.
Medicare Physician Fee Schedule: The system CMS uses to determine payment rates for physician services under Medicare. Updated annually, with recent years showing consistent cuts.
Scope of Practice: The legal definition of what services a healthcare professional can provide. Scope expansion bills allow non-physician clinicians to perform services previously restricted to physicians.
LCME (Liaison Committee on Medical Education): The accrediting body for medical schools in the US and Canada. The AMA is a sponsoring organization.
Prior Authorization: The requirement that physicians get approval from insurance companies before providing certain treatments or services. A major source of administrative burden.
SOURCES
OpenSecrets. American Medical Association Lobbying Profile. OpenSecrets.org, 2024.
American Medical Association. Form 990. Filed November 11, 2025. Fiscal Year 2024.
Centers for Medicare & Medicaid Services. Medicare Physician Fee Schedule Final Rules. 2020-2025.
American Medical Association. AMA Physician Practice Benchmark Survey. 2012-2024.
Physicians Advocacy Institute. Physician Employment Trends. 2024.