
Baylor Scott & White Collects $1.9 Billion in Public Money Every Year. Less Than 1 Percent Goes to Community Health.
Federal Medicare adjustments, Texas Medicaid supplemental payments, 340B drug spread, and four layers of tax exemption. The total public subsidy to Baylor Scott & White is HUGE!

Yesterday, we showed you that four Baylor Scott & White hospitals were running a combined $136 million in annual fair-share deficits.
Today, we show you where that $136 million comes from.
Baylor Scott & White Health collects approximately $1.9 billion in federal and state public subsidies every year.
The CEO collects $10 million.
At the flagship Dallas hospital, $2.6 million of $292 million in reported “community benefit” actually goes to community health improvement.
Less than one percent.
The IRS still calls this a charity.
IN TODAY’S ARTICLE:
The four-pillar subsidy stack: $1.9 billion in public money flowing to BSW annually
The community benefit defense and why the numbers expose it
The LPPF financial engineering that turns $57 million into $642 million
What other state attorneys general have done and what Texas has not
Glossary at the bottom of today’s article.
THE CALLBACK
Yesterday’s article ended with four Baylor Scott & White hospitals among the 10 largest fair-share deficits in Texas. Baylor University Medical Center Dallas at $65 million per year. The Heart Hospital Plano at $32 million. Heart and Vascular Dallas at $20 million. Grapevine at $19 million.
Combined: $136 million per year.
That figure measures the public’s tax-exempt value extended to four BSW hospitals, minus what those four hospitals delivered in meaningful community investment.
The deficit number tells you the gap.
It does not tell you the scale of what flows in.
This article tells you the scale.
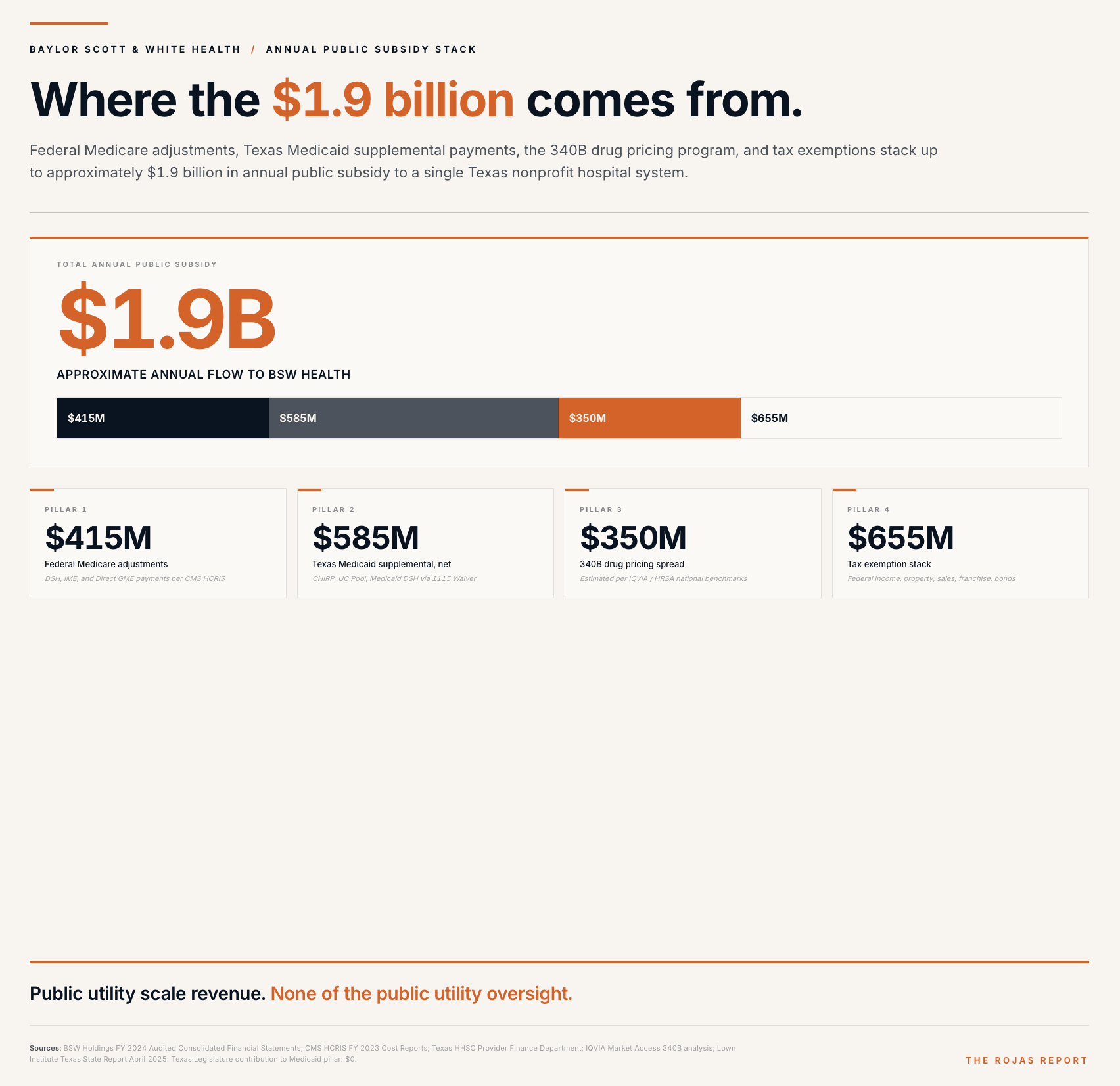
THE STACK
Baylor Scott & White Health collects public money through four distinct pillars. Each pillar represents a federal or state subsidy program. Together, they form the subsidy stack.
Pillar one: federal Medicare adjustments.
Medicare pays BSW hospitals base rates for treating Medicare beneficiaries. In addition to those base rates, BSW collects three supplemental adjustments.
Medicare Disproportionate Share Hospital payments worth approximately $150 million per year, paid to hospitals that serve a high percentage of low-income patients.
Indirect Medical Education payments worth approximately $220 million per year, paid to teaching hospitals to compensate for the indirect costs of training residents. Direct
Graduate Medical Education payments worth approximately $45 million per year, reimbursing the direct salary and benefit costs of resident training.
Federal Medicare add-on subsidies to BSW: approximately $415 million per year.
Pillar two: Texas Medicaid supplemental and directed payments.
Texas operates a complex network of supplemental Medicaid programs authorized under the federal 1115 Waiver.
The largest is the Comprehensive Hospital Increase Reimbursement Program (CHIRP). The state operates CHIRP at $6.5 billion across all participating hospitals for the state fiscal year 2025. BSW reports $88 million in CHIRP receipts for its North Texas hospitals and $69 million for its Central Texas hospitals.
Additional programs include the Uncompensated Care Pool, valued at approximately $157 million to BSW, and Medicaid Disproportionate Share Hospital payments, valued at approximately $35 million. The Uncompensated Care Pool partially reimburses hospitals for the cost of treating uninsured patients.
State Medicaid supplemental payments to BSW: approximately $642 million per year gross.
Pillar three: the 340B drug pricing program.
340B is a federal program that allows qualifying hospitals to purchase outpatient drugs at deep discounts, averaging 55 percent off the wholesale acquisition cost. Hospitals then dispense those discounted drugs to all outpatient prescriptions, including for commercially insured patients. The insurance company pays the full contractual rate. The hospital pockets the spread.
The program was designed to stretch federal resources to reach more low-income patients. The actual outcome is that the largest beneficiaries of the 340B program are major teaching hospital systems with contract pharmacy networks in affluent areas.
BSW operates multiple 340B-eligible hospitals, including BUMC Dallas, BSW Temple, and BSW All Saints. The system maintains an extensive network of contract pharmacies.
Estimated annual 340B benefit to BSW: approximately $350 million.
Pillar four: the tax exemption stack.
As a 501(c)(3) nonprofit, BSW does not pay federal corporate income tax on its operating surplus. BSW reported $1.95 billion in revenue and gains in excess of expenses in fiscal year 2024. A for-profit corporation with the same financial result would face an estimated $400 million federal tax liability.
BSW does not pay local property tax on hospital real estate, with an estimated value of $120 million per year.
BSW does not pay Texas sales tax on most purchases and does not pay Texas franchise tax on operating revenue, estimated combined value: $110 million per year.
BSW borrows capital through tax-exempt municipal bonds at lower interest rates than for-profit competitors. BSW receives tax-deductible charitable contributions from private donors. Estimated combined value: $25 million per year.
Total tax exemption value: approximately $655 million per year.
The stack:
Federal Medicare: $415 million.
State Medicaid supplemental: $642 million gross.
340B drug pricing: $350 million.
Tax exemptions: $655 million.Total: approximately $2.06 billion gross.
Approximately $1.9 billion net of the LPPF self-financing described below.
THE COMMUNITY BENEFIT DEFENSE
Baylor Scott & White and the broader hospital lobby have a standard response to fair share deficit analysis. They argue that the Lown Institute methodology excludes too much of what hospitals do. The Lown methodology counts financial assistance, subsidized health services, community health improvement, and community-building activities. It does not count Medicare and Medicaid underpayment shortfalls. It does not count medical education. It does not count clinical research.
The hospital lobby argues this is unfair. Teaching hospitals carry the cost of training the next generation of physicians. Safety-net hospitals bear the cost of accepting Medicaid patients at below-cost reimbursement rates. These costs are real. The hospital lobby argues they count as community benefit.
The state of Texas agrees with the hospital lobby.
Most physicians have an opinion on nonprofit hospital subsidies.
Very few have read the cost report.
This is where the receipts live: Subscribe
