
CMS Has Opened a New RFI on Physician-Owned Hospitals and TEAM

The FY2027 IPPS proposed rule contains a Request for Information on voluntary physician-owned hospital participation in TEAM. Comments close on June 9, 2026 at 5 p.m. EDT. The eight questions CMS is asking are the entire battlefield.
IN TODAY’S ARTICLE
CMS just asked whether Section 1115A can crack the door Section 6001 closed fifteen years ago.
Three of the eight RFI questions decide whether the opening is real or decorative.
BCBSA already wrote the frame that would exclude surgical-specialty physician-owned hospitals. AHA and FAH file next.
Comments close 5 p.m. EDT on June 9, 2026. Silence is a position.
Glossary at the bottom of today’s article.
Fifteen years ago, the American Hospital Association and the Federation of American Hospitals sold Congress a story. Physician-owned hospitals were cherry-picking patients. Specialty facilities were cream-skimming DRGs. Physician entrepreneurship was threatening the community safety net. The cartel’s lobbying arms spent 2010 writing their competition out of the Medicare program and stitched the result into Section 6001 of the Affordable Care Act.
It worked. Section 6001 froze new physician-owned hospitals out of Medicare participation. The law capped existing facilities at their 2010 bed counts and operating room counts. The physicians who still wanted to own their own facilities watched fifteen years of their careers pass while the same hospital systems that lobbied for the ban spent those years acquiring physician practices, closing rural facilities, and jacking up commercial prices across every market they dominated.
That’s the deal the cartel got from Congress in 2010. On Friday, April 10, 2026, CMS displayed a proposed rule that asks whether the deal gets rewritten.
What CMS actually did
CMS displayed CMS-1849-P, the FY2027 Inpatient Prospective Payment System proposed rule, on April 10, 2026. The Federal Register published it on April 14. Inside the section on the Transforming Episode Accountability Model, CMS included a Request for Information with eight questions. The questions ask whether CMS’s Innovation Center should allow physician-owned hospitals to voluntarily opt into TEAM, and whether Section 1115A demonstration authority should waive specific provisions of Section 6001(a)(3) to make that opt-in operational.
Congress enacted both Section 1115A and Section 6001 as part of the Affordable Care Act in 2010. Same law. Section 6001 closed the door on physician hospital ownership. Section 1115A granted the CMS Innovation Center authority to waive Medicare statute for demonstration models. Fifteen years later, CMS is asking whether Section 1115A can reach Section 6001(a)(3). The same statute that closed the door is being asked whether it can crack the door open.

The statutory expansion-exception process under Section 6001 is narrow. It has not produced broad reopening. Repeated legislative efforts to loosen or repeal the restrictions have not produced broad reopening either. Three bills currently sit in the 119th Congress. H.R. 4002 would repeal Section 6001 entirely. H.R. 2191 and S. 1390 would create a rural carve-out. An eighty-eight organization coalition including physicians, payers, and patients supports the rural bill. None has moved.
This RFI is different. It places an administrative opening on the public record. Comments close at 5 p.m. EDT on June 9, 2026. The final rule is expected in August.
TEAM itself is a five-year mandatory bundled payment model that started January 1, 2026. It covers five surgical procedures. Coronary artery bypass graft. Lower extremity joint replacement. Major bowel procedure. Surgical hip and femur fracture treatment. Spinal fusion. According to Physician-Led Healthcare for America, approximately fifteen physician-owned hospitals are already mandated into TEAM because CMS selected their Core-Based Statistical Areas for the model. The RFI is about whether to open voluntary opt-in to physician-owned hospitals in CBSAs that were not selected.
The door cracked. The cartel is already writing the frame that would narrow what gets through it.
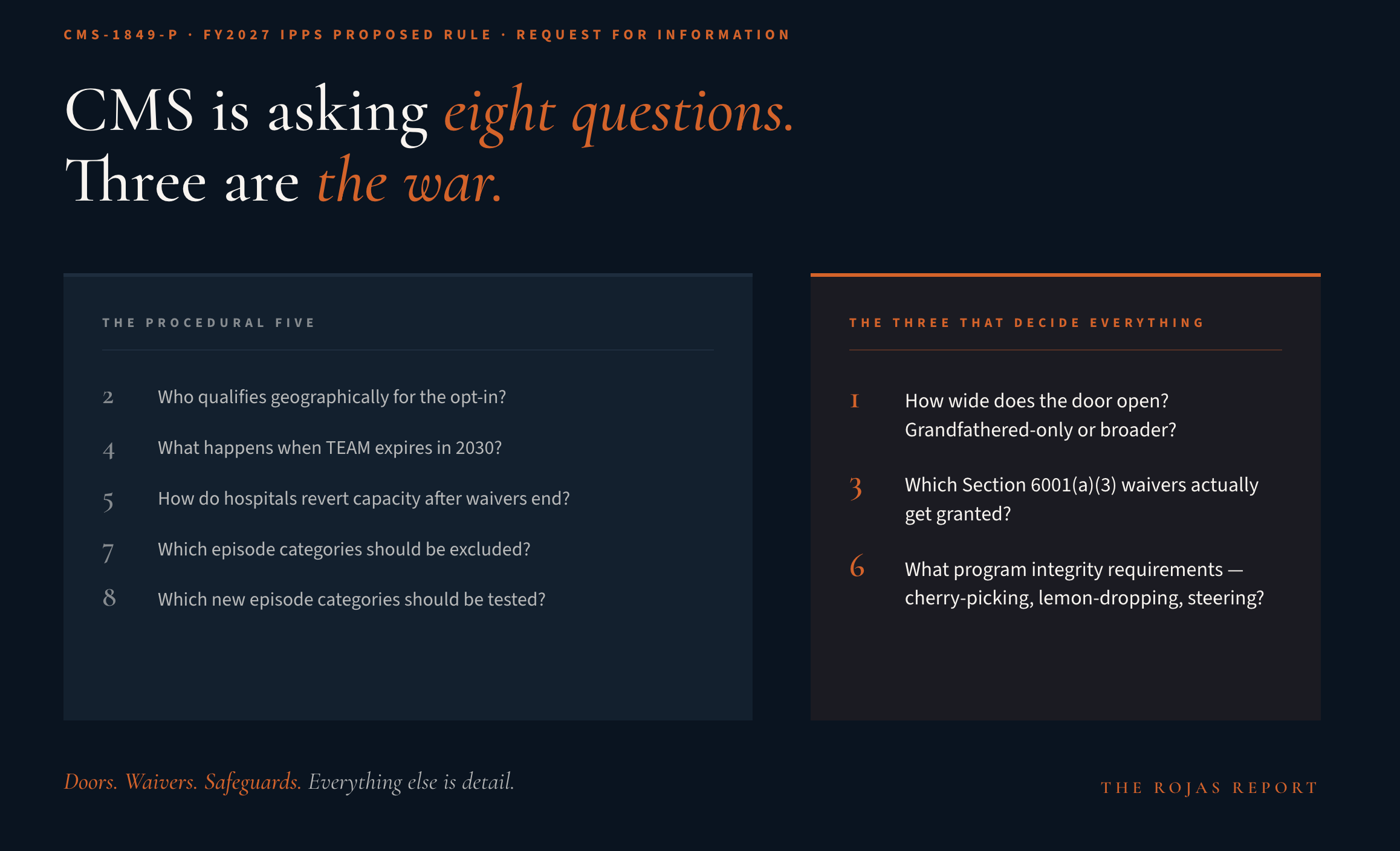
Question 1: How wide does the door open?
CMS asks whether to allow a voluntary opt-in period, and whether participation should be limited to physician-owned hospitals grandfathered under the ACA to use the rural provider or whole hospital exception to the physician self-referral law.
This is door width.
It controls everything downstream.
Grandfathered-only limits opt-in to physician-owned hospitals that existed and participated in Medicare before December 31, 2010. That’s the narrow path. It treats the RFI as a payment model adjustment for the existing grandfathered class. No new entrants. No expansion of physician hospital ownership beyond what survived the ban.
The broader path treats the RFI as what it actually is. A question about whether Innovation Center demonstration authority creates Medicare participation opportunities for physician-owned hospitals that did not exist or could not participate in 2010. That opens TEAM to new entrants. It creates a pathway where none has existed for fifteen years.
Watch what AHA and FAH file on this. They’ll argue Section 6001 was Congressional intent. They’ll argue CMMI lacks authority to undo Congressional intent through demonstration models. They’ll ask CMS to limit opt-in to grandfathered hospitals only. That restriction renders the RFI essentially symbolic. A payment model tweak for the existing class and nothing else.
The physician-led position is that Section 1115A is explicit, broad, and designed exactly for questions like this. Testing whether physician-owned hospitals deliver bundled episode care at lower cost and equal or better quality requires physician-owned hospitals in the test. Limiting opt-in to grandfathered facilities limits the test to a pre-selected population already operating under structural constraints that non-grandfathered physician-owned hospitals do not face. The comment docket needs sustained pressure arguing the opt-in must be available to any physician-owned hospital meeting programmatic requirements, grandfathered or otherwise.
Question 2: Who qualifies geographically?
CMS asks whether opt-in physician-owned hospitals need to meet the same geographic eligibility criteria as other TEAM participants under 42 CFR 512.515, and whether additional inclusion criteria should apply.
The geographic question looks procedural. It is not.
If the opt-in is geographically limited to CBSAs where TEAM already operates, the addition is trivial. Those markets already contain the approximately fifteen mandated physician-owned hospitals PHA identified. If the opt-in extends to physician-owned hospitals in any CBSA, the model grows meaningfully and the test produces more useful data.
The additional inclusion criteria language is where the cartel hides exclusions inside safeguards. Watch for proposals to exclude physician-owned hospitals with case volume below a minimum threshold, with specialty concentration above a threshold, or outside specific urbanicity bands. Each exclusion narrows the opening without appearing to oppose it directly. The cartel counts on complexity to hide in plain sight.
The physician-led position is that geographic eligibility matches TEAM’s existing criteria without additional restriction. Inclusion criteria focus on quality metrics and participation capacity, not structural characteristics that exclude legitimate facilities from competition.
Question 3: Which waivers actually get granted?
CMS asks what programmatic waivers are necessary for physician-owned hospital participation. Expansion restrictions. Service limitations. The agency asks commenters to justify each waiver and explain how it will not undermine the model by allowing Medicare payment for services where payment is not currently allowed.
This is the operational question. It determines whether the opening is real or decorative.
Section 6001(a)(3) contains multiple operational constraints. The bed count cap. The operating room cap. The procedure room cap. The expansion request process through the Secretary. The ownership percentage freeze. The disclosure requirements. CMS is asking which of these to waive.
A narrow waiver list produces a hollow opening. Waive only the procedural requirement to request expansion through the Secretary, retain the bed count cap and the operating room cap, and the opt-in facility cannot actually scale operations to take on additional TEAM episodes. The hospital holds a theoretical right to participate and a practical impossibility to do so.
A meaningful waiver list addresses the operational constraints that actually prevent physician-owned hospital growth. Bed counts. Operating rooms. Procedure rooms. Service line restrictions. The expansion approval process. Every provision must be named specifically in comments, with justification showing why participation in TEAM cannot succeed without the waiver.
The trap in Question 3 is the burden of proof. CMS asks commenters to justify each waiver against the concern of allowing Medicare payment for services Section 6001 otherwise disallows. That framing treats every waiver as a deviation from baseline Congressional intent. The physician-led response flips the framing. Section 1115A exists precisely to test payment authorities that statutory default prohibits. The entire purpose of Innovation Center demonstration authority is to waive provisions to determine whether alternative structures produce better outcomes. The burden of proof belongs on the model design, not the waiver requests.
Context for Question 3 arrived eleven months before CMS filed the rule.
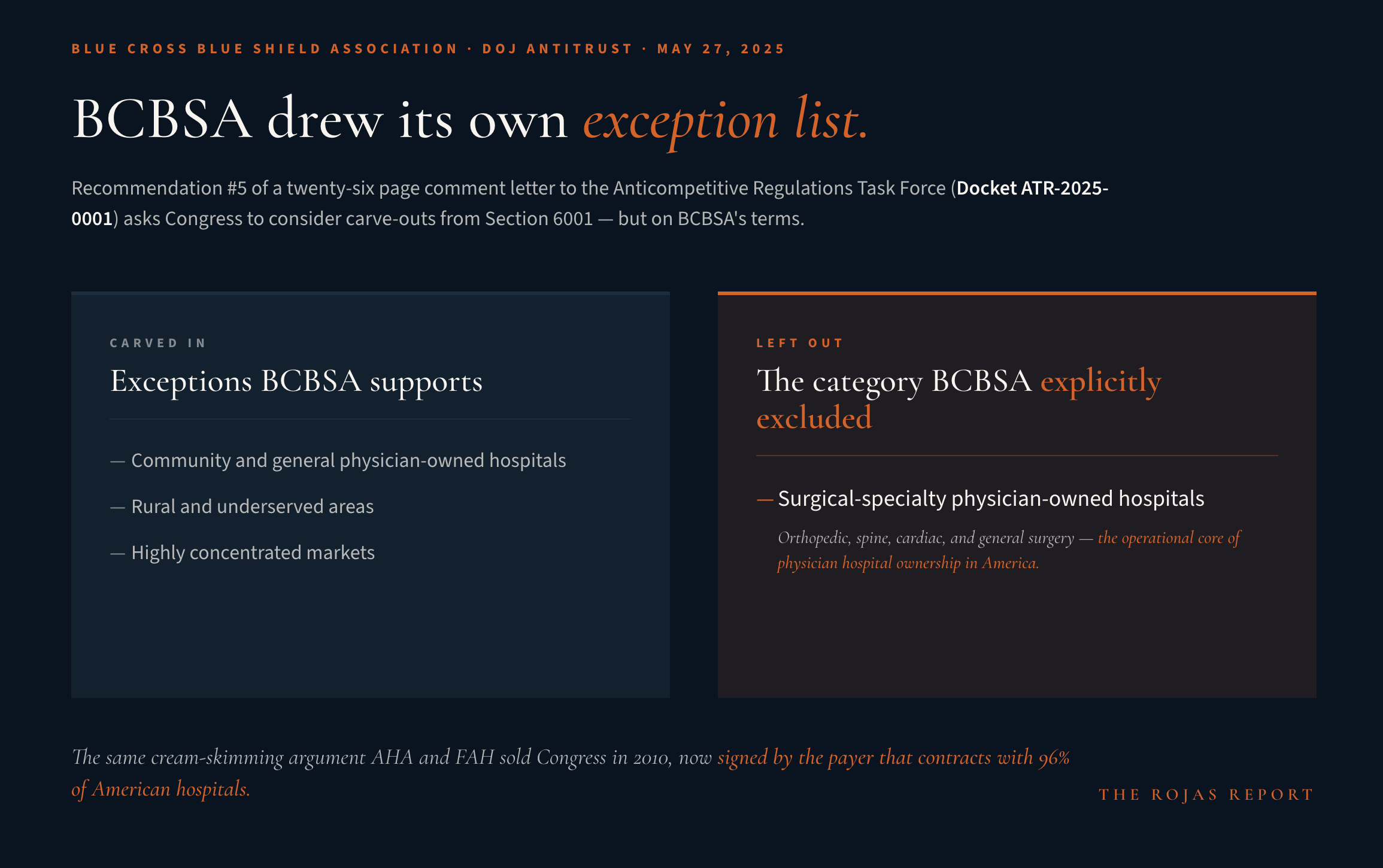
On May 27, 2025, the Blue Cross Blue Shield Association submitted a twenty-six page comment letter to the Department of Justice Antitrust Division’s Anticompetitive Regulations Task Force, Docket ATR-2025-0001. Anshu Choudhri, BCBSA’s Vice President of Policy Development, signed the letter. A payer that contracts with 96 percent of American hospitals and covers one in three Americans put itself on the federal record asking for exceptions to the Section 6001 ban.
Recommendation #5 of that letter cites Social Security Act §1877, the statute Section 6001 amended. It asks Congress to consider exceptions to restrictions on physician-owned hospitals when the goal is to improve competition and patient choice.
That’s the pressure signal. The payer that cracked the door is real. The payer also proposed the terms. BCBSA recommended carve-outs for community and general physician-owned hospitals. Rural and underserved areas. Highly concentrated markets. The letter explicitly excluded surgical-specialty physician-owned hospitals from its proposed exceptions. BCBSA’s stated concern, verbatim from the letter: “There is a concern that the latter type of POH could target patients and services with higher cost diagnosis-related groups (DRGs) with more favorable margins. This could leave non-POHs with the liability to provide access to emergency room, maternity and other services with lower margin DRGs.”
That’s the cream-skimming argument. It’s the same argument AHA and FAH used to sell Section 6001 to Congress in 2010. The 2023 Physicians Advocacy Institute and Physicians Foundation study analyzed approximately 740,000 Medicare discharges across 186 physician-owned hospitals and found patient age, race, ethnicity, and comorbid conditions virtually identical between physician-owned and traditional hospitals in the same geographic areas. The cream-skimming claim has been studied. It has not held up to the data.
The vocabulary also appeared in BCBSA’s May 2025 letter, but CMS had already used similar language in earlier physician-owned-hospital rulemaking. Beneficiary steering. Cherry-picking. Lemon-dropping. Three words the cartel has carried inside federal rulemaking for years. BCBSA reinforced the frame. CMS had already been operating inside it.
Surgical-specialty physician-owned hospitals are the operational core of physician hospital ownership in America. Orthopedic, spine, cardiac, and general surgery specialty facilities are what physicians can build without acute-care infrastructure and systems-scale capital. They’re also the category BCBSA explicitly excluded from its proposed exceptions. If the final rule adopts BCBSA’s framing on specialty facilities, the opt-in becomes a narrow pathway for community hospitals in rural areas. The specialty facilities where the majority of physician hospital ownership actually operates stay exactly where Section 6001 left them in 2010. Frozen. Waiting to be acquired by the systems that lobbied for the ban.
The comment docket addresses this directly or the opening closes.
What physicians do before June 9
The comment docket is not the battlefield.
The silence of physicians who own and operate these hospitals is.
Lobbyists will file. AHA will file. FAH will file. BCBSA will file, in more polished form than its May 2025 DOJ letter. PHA will file on behalf of the coalition. The AMA will file. Every trade association in healthcare will produce a comment letter, and most of those letters will cancel each other out.
What has not happened is the physicians themselves speaking on the public record in volume. Not their trade associations. Not their lobbyists. Them.
Every surgeon who operates in a physician-owned hospital. Every physician who wanted to build one and was stopped by Section 6001. Every clinician who watched a colleague’s practice get absorbed by the health system that lobbied for the ban fifteen years ago. All of them have what the cartel’s lawyers do not. Names. Faces. Operating rooms. Patients. Fifteen years of direct experience with what the ban did to American medicine.
Here’s what to do.
Record a sixty-second video. Say who you are, where you practice, why Section 6001 has constrained your ability to build the hospital your patients deserve, and what you want CMS to do. Post it to X, LinkedIn, and Instagram. Tag @CMSinnovates and @HHSGov. Use #PhysicianLedCare and #Section6001.
Submit a comment at regulations.gov. Reference file code CMS-1849-P. Do it before 5 p.m. EDT on June 9, 2026. The comment does not have to be long. It has to be on the record. Eight questions. Your answer to any of them, in your own language, from your own experience, carries more weight than another lobbyist memo.
The last fifteen years of physician hospital ownership were decided by the people who filed comments.
The next fifteen get decided the same way.
Not filing is filing.
Keep reading with a 7-day free trial
Subscribe to The Rojas Report to keep reading this post and get 7 days of free access to the full post archives.