
Co-opetition Is the Next Stage of American Capitalism
I interviewed 71 independent practices. Not one collaborated to reduce overhead. That's the gap we're fixing.

There’s something strange about American healthcare that we’ve all been trained not to notice.
If you buy a cup of coffee from an independent café, it costs roughly the same as one from a chain. Sometimes less.
The beans don’t suddenly become more expensive because Starbucks bought the shop.
In healthcare, the opposite is true.
When a hospital system acquires an independent clinic, the same service, performed by the same doctor, in the same building, with the same equipment, can legally cost 50% to 165% more.
Nothing changed except the Tax Identification Number.
That isn’t pricing. It’s arbitrage.
The Game CMS Built
Over the last 28 years, the Centers for Medicare & Medicaid Services quietly rewired incentives in American healthcare.
They did two things at the same time:
Lowered professional fees (what physicians are paid)
Raised facility fees (what hospitals are paid)
Originally, facility fees applied only to hospitals and ambulatory surgery centers.
Two buildings.
Two schedules.
Today, if a nonprofit health system acquires a primary care clinic and designates it a “provider-based department,” it can add a facility fee to every visit.
This change took effect with revisions to specific CMS regulations. To help clarify the impact, imagine a brief snapshot of the situation before and after the CMS rule change:
Before the CMS rule revision, hospitals and ambulatory surgery centers were the primary entities charging facility fees, creating a dual schedule. However, the rule allowed non-hospital clinics to levy similar fees if acquired and designated appropriately.
As a result, what was once a $65 primary care appointment could become $190 overnight. Same doctor. Same room. Same care. This sudden increase in revenue highlights the significant financial incentives arising from the policy change.
That delta isn’t value creation. It’s policy-engineered arbitrage, and it’s the economic engine behind physician consolidation.
The 12% Problem
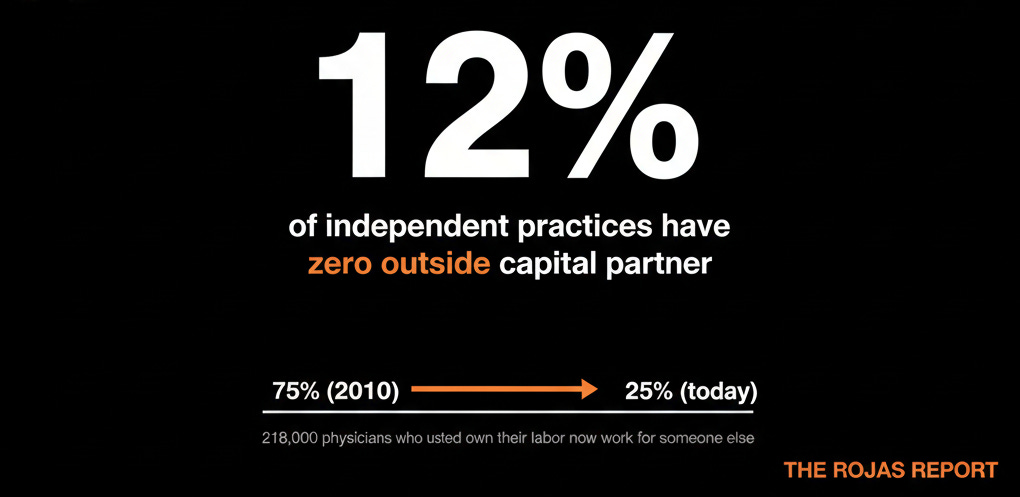
In 2010, roughly 75% of physicians worked in private practice.
Today, it’s less than 25%.
A recent study showed something even more alarming: Only 12% of independent practices in the U.S. have no outside capital partner, no private equity, no health system joint venture.
That represents 218,000 physicians who used to own their labor and now work for someone else.
This isn’t good for employers.
It isn’t suitable for patients.
And it isn’t good for physician supply.
But it’s incredibly good for the systems doing the acquiring.
The Rojas Report is healthcare’s independent voice.
Just the economics of American healthcare: who wins, who pays, and what the independent physician can do about it. If that’s the kind of work worth supporting, I’d be honored to have you subscribe.
