
Congress Doesn't Subsidize Healthcare. Congress Subsidizes the Cartel.
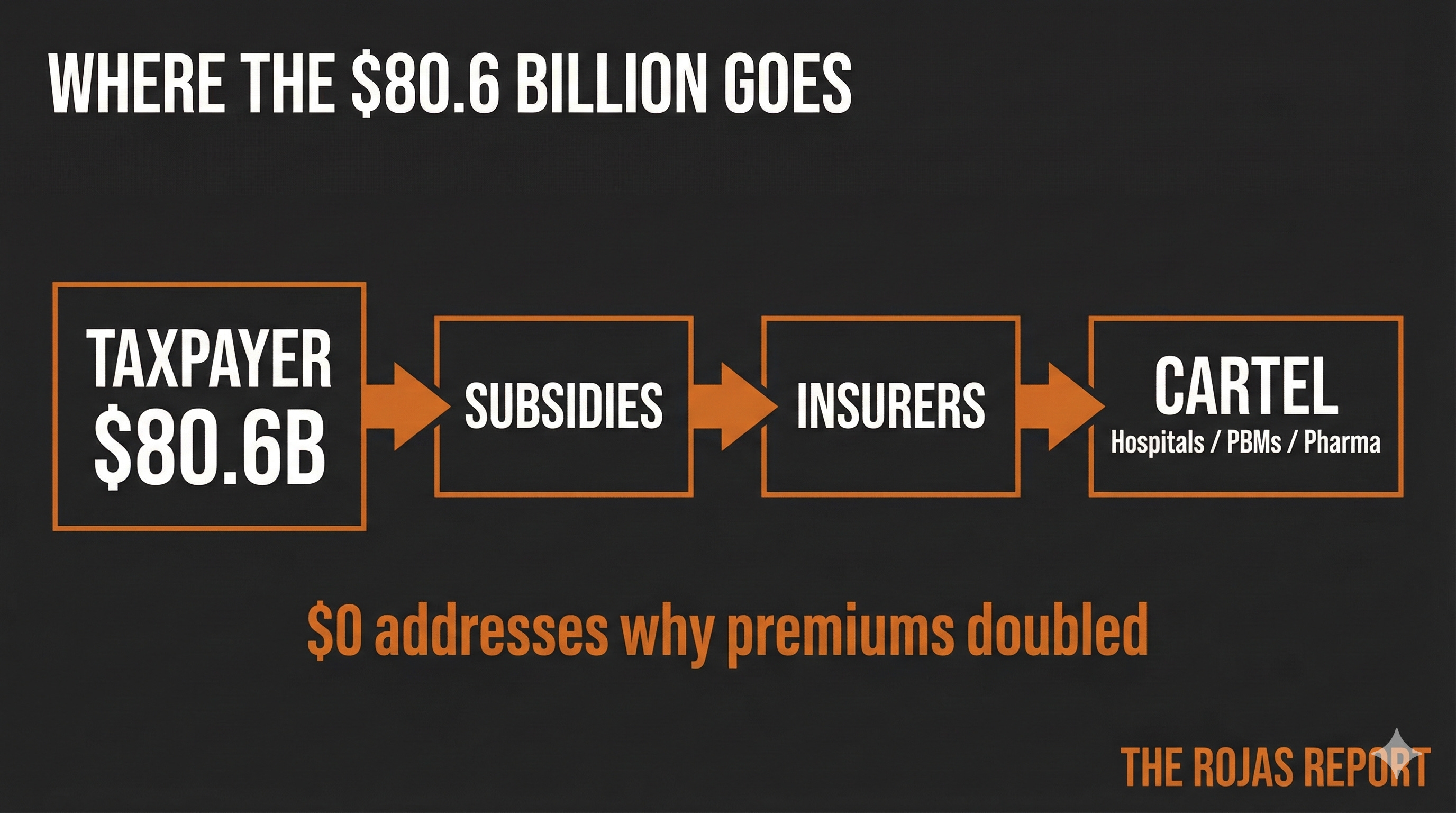
The House just voted to spend $80.6 billion extending ACA subsidies. Not one dollar addresses why premiums doubled. That's the point.

The House just passed an $80.6 billion bill to extend ACA subsidies.
Republicans called it a betrayal.
Democrats called it a victory.
Neither party asked the only question that matters:
Why do premiums double without government money propping them up?
Does answering that question would expose the entire game?
IN TODAY’S ARTICLE:
Why both parties agreed to subsidize premiums instead of fixing prices
The 17 Republicans who crossed party lines to protect hospital bad debt exposure
CMS site-neutral changes that actually threaten hospital revenue (and why Congress ignores them)
The 340B survey, the FTC’s PBM case, and the regulatory moves Congress ignores
Glossary at the bottom of today’s article.
AUDIO VERSION
🎧 Audio version available below.
THE VOTE THAT PURCHASED NOTHING
The House passed the ACA subsidy extension 230-196.
17 Republicans joined all Democrats. They used a discharge petition to force the vote. GOP leadership opposed it. It passed regardless.
The bill extends enhanced premium tax credits for three years. The CBO estimates $80.6 billion in cost. 4 million more Americans insured by 2028.
Senate GOP leaders declared it dead on arrival.
Without action, approximately 22 million ACA enrollees will face average premium increases of 100% or more.
That’s the news.
Here’s what the news doesn’t tell you:
Not one dollar of that $80.6 billion addresses why premiums require subsidies to be affordable.
Not one provision touches hospital pricing.
Not one provision addresses physician ownership restrictions.
Not one provision repeals Certificate of Need laws.
Not one provision challenges PBM rebate extraction.
Not one provision asks why ACA marketplace premiums doubled since 2014.
The subsidy extends the cover-up. It doesn’t fix the crime.
THE BIPARTISAN CONSENSUS
Republicans want to end the subsidies.
Democrats want to extend them.
This looks like disagreement.
It is actually consensus.
Both parties agree on the fundamental premise: healthcare costs are immovable, and the only political question is who pays the bill.
Republicans say the patient pays.
Democrats say the taxpayer pays.
Neither party says the bill is fraudulent.
The premium subsidy debate is a performance.
Two parties arguing over who holds the bag while the cartel fills it.
The 17 Republicans who crossed party lines didn’t rebel against their ideology.
They protected their districts.
Their hospitals.
Their health systems’ balance sheets.
They will receive their due renumeration.
22 million people losing subsidies means 22 million people who can’t pay hospital bills. That’s not a patient crisis.
That’s a bad debt crisis.
Those 17 Republicans did the math.
Their hospital CFOs did it first.
This is how the cartel operates.
It holds patients hostage, then bills the taxpayer for the ransom.
The healthcare cartel counts on you not paying attention.
60,000+ physicians refuse to comply.
Join them.
THE FREE MARKET SOLUTIONS THAT REMAIN ILLEGAL
Here’s what Congress could do tomorrow:
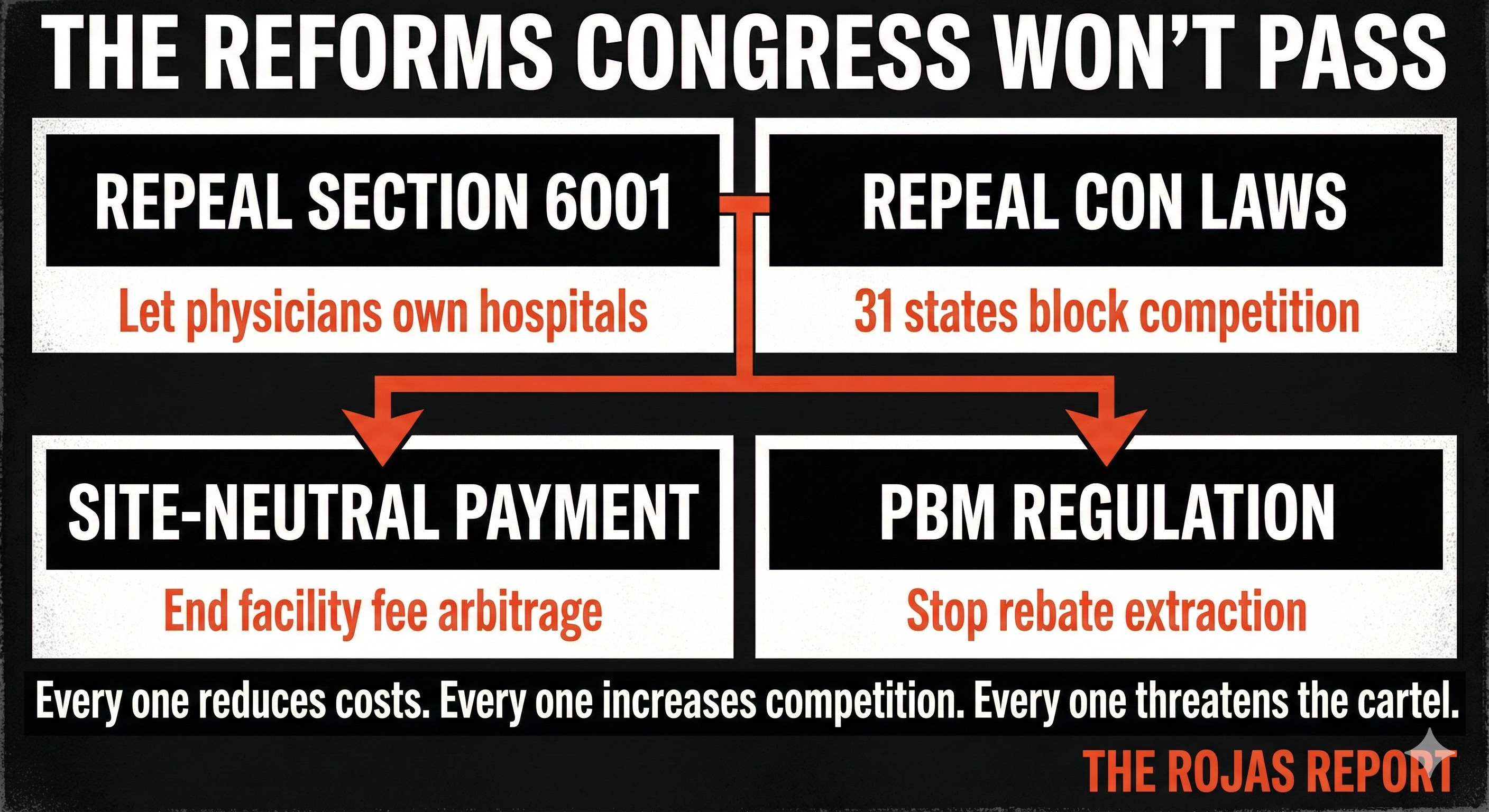
Repeal Section 6001. Let physicians own hospitals again. Before the 2010 ban, physician-owned hospitals had better outcomes, lower costs, and higher patient satisfaction. Congress banned them because they competed too effectively.
Repeal Certificate of Need laws. 31 states require permission from incumbent hospitals to build new facilities. The incumbents sit on the approval boards. Competition is illegal by design.
Pass site-neutral payment reform. Hospitals charge 2-3x more than independent physicians for the same service. The facility fee is pure extraction. Congress knows this. Congress does nothing.
Regulate PBM rebates. Pharmacy Benefit Managers extract billions in rebates that never reach patients. The FTC is investigating. Congress watches.
Every one of these reforms would reduce costs. Every one would increase competition. Every one would threaten the cartel.
Congress subsidizes instead.
The $80.6 billion isn’t healthcare policy. It’s protection money.
The healthcare system rewards those who understand it and punishes those who don’t. There’s no middle ground.
WHAT’S ACTUALLY HAPPENING (WHILE CONGRESS PERFORMS)
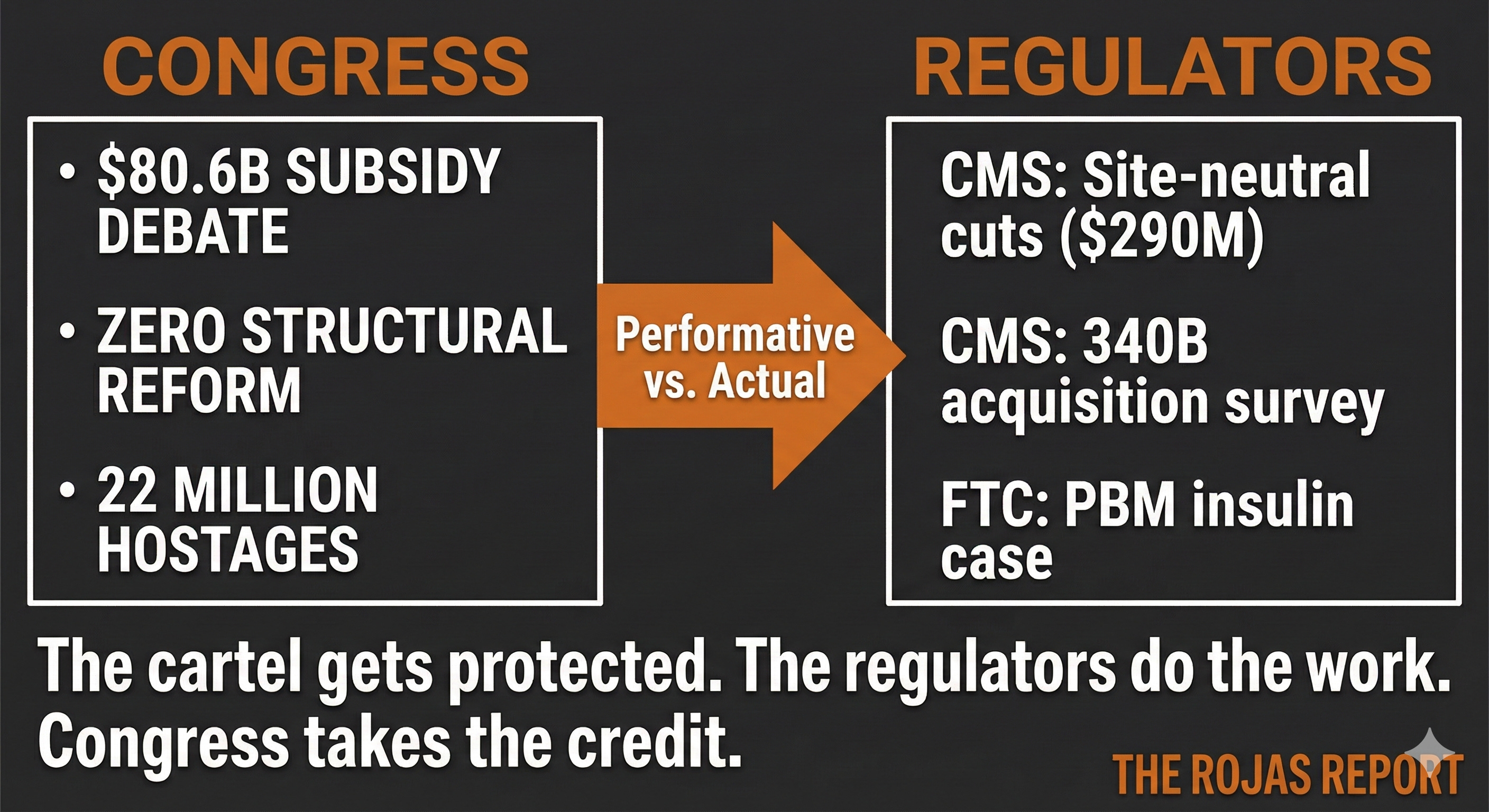
While the House staged its subsidy theater, actual policy changes moved forward. None of them originated in Congress.
CMS Site-Neutral Drug Administration Payments
Effective January 1, 2026, CMS cut payments for drug administration at off-campus hospital outpatient departments to 40% of the hospital rate. These facilities now receive payments equivalent to the physician fee schedule.
Estimated reduction: $290 million in 2026.
CMS exempted Rural Sole Community Hospitals.
CMS signaled this is the beginning. Larger site-neutral expansion to on-campus settings and imaging is coming in future rulemaking.
This is a direct hit on facility fee arbitrage. Hospitals spent two decades buying physician practices and repricing their services at hospital rates. CMS is starting to close that gap.
Congress didn’t do this. CMS did. Congress won’t touch it.
CMS Drug Acquisition Cost Survey
Also effective January 1: CMS launched a survey requiring all OPPS hospitals to report what they actually pay for outpatient drugs. Net of rebates. Net of discounts.
The survey runs through March 31.
Results will inform the 2027
OPPS proposed rule.
Why this matters: 340B hospitals.
CMS postponed the accelerated 340B remedy offset. The 0.5% reduction stays for 2026. But CMS signaled a 2% or higher reduction starting in 2027.
340B hospitals receive deeply discounted drugs and bill insurers at full price. The spread is substantial. CMS is gathering the data to quantify it.
When that data goes public, the 340B program’s political cover evaporates.
Congress created 340B. Congress refuses to reform it. CMS is doing the work Congress won’t do.
FTC PBM Insulin Case Proceeds
The FTC’s administrative case against Caremark, Express Scripts, and OptumRx continues.
The PBMs moved to dismiss on August 29, 2025. They argued the FTC failed to define the relevant market or allege actual competitive harm.
The Administrative Law Judge lifted the stay in August 2025. The court has not set an evidentiary hearing timeline.
This case matters. The FTC alleges that the three largest PBMs coordinated to inflate insulin prices through rebate structures that punished lower list prices. If the FTC wins, the PBM business model faces existential threat.
Congress could regulate PBMs tomorrow.
Congress doesn’t.
The FTC acts alone.
THE PATTERN
Congress debates subsidies.
CMS moves on site-neutral.
The FTC pursues PBMs.
The structural changes happen around Congress.
Despite Congress.
While Congress performs outrage about premium costs it refuses to address.
22 million Americans held hostage.
$80.6 billion in ransom.
No structural reform.
The cartel wins again.
The free market solutions exist.
They sit in legislative graveyards.
Physician hospital ownership.
CON repeal.
Site-neutral payment.
PBM regulation.
Every one illegal, restricted, or blocked.
The subsidy isn’t healthcare.
The subsidy is the cover-up.
And every few years, both parties perform their roles.
Republicans threaten to expose the real prices.
Democrats promise to keep them hidden.
The taxpayer pays.
The patient stays hostage.
The physician stays locked out.
The cartel extracts.
Nothing changes.
Until we build the alternative.
-Rojas out.
GLOSSARY
Premium Tax Credits (ACA Subsidies): Federal payments that reduce monthly health insurance premiums for ACA marketplace enrollees. Available on a sliding scale based on income. Enhanced credits expanded in 2021, scheduled to expire without extension.
Discharge Petition: A procedural tool allowing House members to force a floor vote on legislation that leadership has blocked. Requires 218 signatures. Rarely successful. Used here to bypass GOP leadership opposition.
Site-Neutral Payment: A policy that pays hospitals and physicians the same rate for the same service, regardless of where it’s performed. Currently, hospitals receive higher rates for services that could be performed in lower-cost settings.
OPPS (Outpatient Prospective Payment System): Medicare’s payment system for hospital outpatient services. Sets standardized rates for procedures and services. Site-neutral reform targets OPPS rates.
340B Program: A federal program requiring drug manufacturers to provide outpatient drugs at significant discounts to eligible healthcare organizations serving low-income patients. Hospitals can bill insurers full price and pocket the spread.
Certificate of Need (CON) Laws: State laws requiring healthcare facilities to obtain government approval before building new facilities, expanding services, or purchasing major equipment. Incumbent competitors often influence approval decisions.
Section 6001: A provision in the 2010 Affordable Care Act that banned Medicare reimbursement to new physician-owned hospitals and restricted expansion of existing ones. Effectively froze physician hospital ownership.
PBM (Pharmacy Benefit Manager): Intermediaries that manage prescription drug benefits for health plans. The three largest (Caremark, Express Scripts, OptumRx) control approximately 80% of the market. The FTC alleges anticompetitive practices.
Facility Fee: An additional charge billed by hospitals for services provided in hospital-owned settings. The same service performed in an independent physician office incurs no facility fee. Site-neutral reform targets this disparity.
SOURCES
Congressional Budget Office. “Cost Estimate: ACA Premium Tax Credit Extension Act.” CBO.gov, January 2026.
Congress.gov. “H.R. 1834: ACA Premium Tax Credit Extension.: ACA Premium Tax Credit Extension.” Roll Call Vote 230-196.
Centers for Medicare & Medicaid Services. “CY 2026 Hospital Outpatient Prospective Payment System Final Rule.” CMS.gov, November 2025.
Centers for Medicare & Medicaid Services. “Drug Acquisition Cost Survey Requirements.” CMS.gov, January 2026.
Federal Trade Commission. “In the Matter of Caremark Rx, LLC, Express Scripts, Inc., and OptumRx, Inc.” Administrative Docket. FTC.gov, August 2025.
After our Governor accepted a billion dollars graciously bestowed on each state for rural healthcare and infrastructure, we couldn’t contain our frustration. Hence, the rant below…
__________
💸 Beleaguered Taxpayer Comments
The nine most terrifying words in the English language are: I'm from the Government and I'm here to help . — President Reagan's famous and prescient quote from August 12, 1986 News Conference: https://www.youtube.com/watch?v=nCedOQJ0ZEA
While legislators ponder daycare fraud, we ask that they also investigate what will happen to all the beautiful taxpayer money Trump's One Beautiful Bill Act (OBBA) will generously gift to "help" rural residents?
As rural Idaho residents, we can tell you that many do not want this "help," which likely will bring more people into once pristine, low-crime areas. Newcomers often demand ever more “citified” services that could destroy rural residents' environment, lifestyle, independence, resilience, and — yes — their health. (Of course, media, politicians, and others who control the purse strings will disagree vehemently.)
Throwing money at "healthcare access, affordability" — with or without accountability safeguards — will not provide healthcare access and affordability any more than throwing money into Obamacare and student loans made healthcare premiums and college more accessible and affordable. Instead, with government (i.e., taxpayer) subsidies, costs went up while access went down. And, of course, strings were attached.
Abuse is inevitable when government sloshes other people's money to bureaucrats, NGOs, health boards, etc. for redistribution to "the underserved." Lots of money gets caught in the middleman's net and often funds solutions that don't work.
🔥 Can't state legislatures JUST SAY NO to federal dollars, pretty please?
P.S. We've watched meetings of Idaho’s Central District Health (CDH), which serves populous Ada County as well as more rural Boise, Elmore, and Valley counties. Many "services" provided are pure socialism or downright dangerous to health; the hearings quite appalled us. CDH meetings on YouTube: https://www.youtube.com/channel/UC4LJ1BM5Jv3zczecnYkXarw
Congress, whether Democrat or Republican, is worthless to the everyday taxpayers. They don’t solve problems. They create them. They they apply other-people’s-money Bandaids, pat us on the head, say “there, there, dear, see, we fixed it” and avoid looking at the gaping wound (aka cartel money pit) that really needs repair.
Thank you for bringing this out into the open. We must stop feeding these beasts, ideally by avoiding the healthcare/insurance/drug cartel system altogether. Except for acute injuries (and some acute diseases), traditional medical care has completely failed us under this system. So let’s dump it altogether. It’s irretrievably broken.