
Doctors Don’t Lose Policy Fights Because They’re Wrong. They Lose Because They Don’t Pay.
The hospital lobby built a political capital stack. Physicians built a complaint habit.

Doctors believe political donations are unseemly.
Hospitals believe political donations are insurance.That is why one side has a federal lobbying machine.
The other side has a fee schedule that gets cut every year.Kevin Hern starts this Senate race with seven million dollars.
The hospital lobby has spent fifty years building the donor pipeline around every committee that touches Medicare. Physicians have built a habit of complaining at conferences.
One of these strategies compounds.
The other gets reimbursed at a lower conversion factor.
THE PROBLEM IS NOT WHAT YOU THINK IT IS
Independent medicine has been losing structural policy fights for thirty years.
The standard explanation is that hospitals have better lobbyists, lawyers, narratives, or connections.
That is not the explanation.
The explanation is simpler. One side made an investment. The other side made a moral statement.
The investment compounded.
The moral statement was cut from the conversion factor every year.
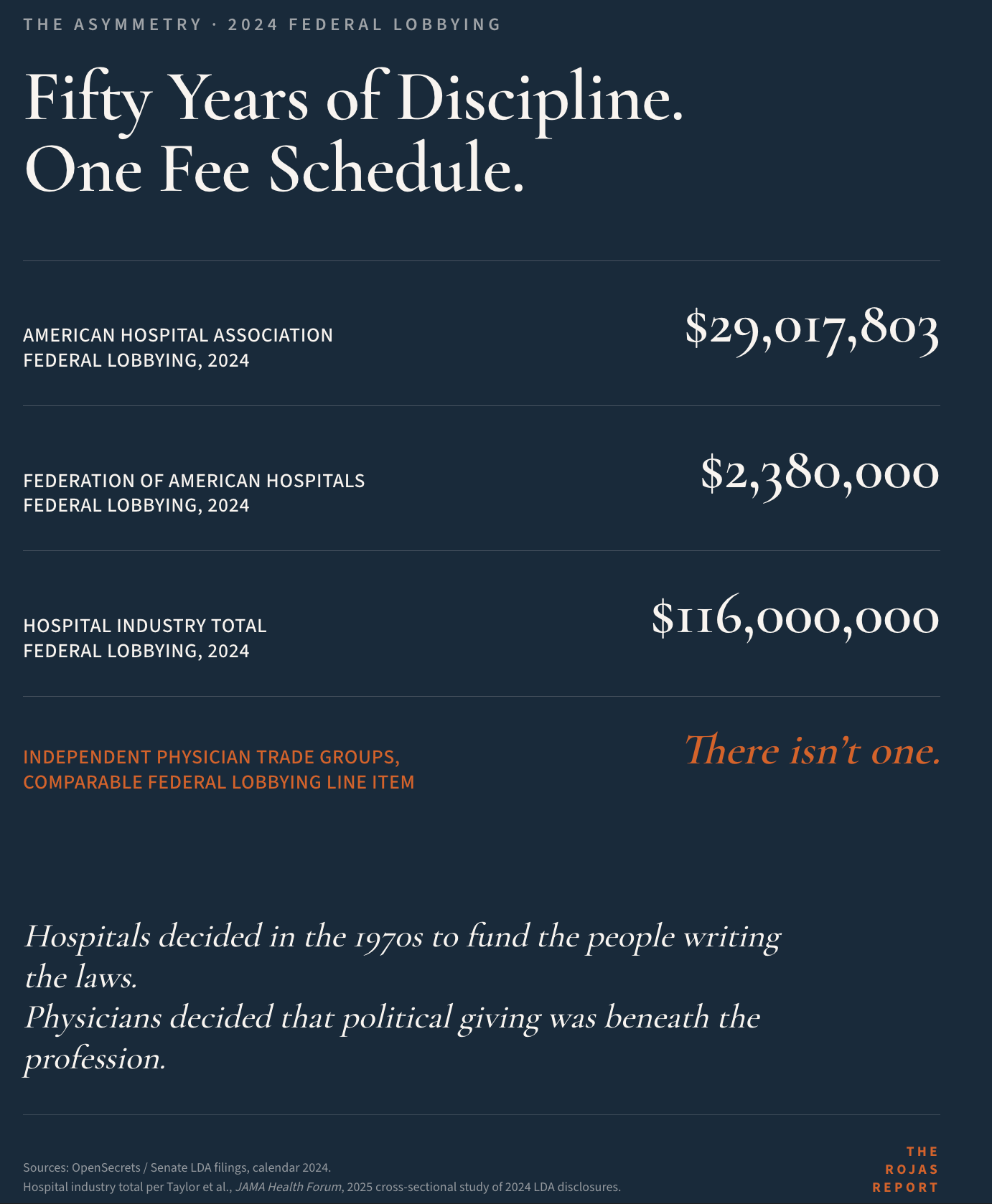
Pull the 2024 federal lobbying disclosures. The American Hospital Association spent $29 million. The Federation of American Hospitals spent $2.4 million. Hospitals and health systems combined spent $116 million.
Independent physician trade groups have no comparable line item. Not “smaller.” Not “less coordinated.” None.
That is the entire architecture in one paragraph.
When the Medicare conversion factor gets cut, hospitals already had eight people in the room arguing for the carve-outs that protect hospital outpatient department reimbursement. Independent physicians had a press release. The carve-outs are written into the rule. The press release is read by other physicians.
This is not a story about who is right. The Avalere data is overwhelming. Independent practices cost Medicare less per beneficiary, drive fewer inpatient days, and generate fewer emergency department visits than hospital-affiliated practices. Researchers published the data. No one contests it. The data did not change the rule.
They didn’t outcompete. They out-lobbied.
You have been complaining about outcomes without funding the inputs that support them.
You can learn how committee math actually works.
Or you can keep being surprised when it works against you.
Subscribe to The Rojas Report at read.rojasreport.com.
THE MECHANISM
Senate Finance has jurisdiction over Medicare, Medicaid, and federal tax policy. CMS writes the annual rule administratively, but Congress sets the conversion factor in statute, and Senate Finance writes the statute. Every meaningful change to physician payment in the last decade ran through that committee.
Site-of-service rules. 340B reform, or the refusal of it. Medicare Advantage payment rates. Alternative payment models. The conversion factor itself.
Hospital donors funded every member of that committee. Pull the FEC reports. AHA is in there. FAH is in there. AAMC is in there. Every regional system in their state is in there.
Pull the FEC reports for independent physicians.
You will not find a comparable line item.
This asymmetry grew over fifty years of consistent hospital donations and physician abstention. One side invested.
Between 2027 and 2030, the same committee will rewrite the conversion factor. It will rewrite site-neutral payment policy. It will rule on the next round of Medicare Advantage reform.
If the donor mix on that committee in 2030 is similar to what it was in 2020, it is likely the rule will remain as it has. Same inputs. Same outputs.
The math problem is not whether physicians’ arguments are correct.
The question is whether physician perspectives are presented to a committee willing to consider them.
THE LIVE TEST CASE
Kevin Hern announced his Senate run on March 11, 2026. He is replacing Markwayne Mullin, who left the Senate to serve as the Department of Homeland Security’s acting secretary.
Hern is in his fourth term in the U.S. House. He sits on Ways and Means. He chaired the Republican Study Committee. He now chairs the Republican Policy Committee.
Before any of that, he ran a McDonald’s franchise group. Eighteen restaurants in the Tulsa metro. He sold the last one in 2021.
That biography matters more than it sounds.
Most senators have never signed a payroll check. Most senators have never priced a menu against a CPI shock. Most senators have never explained to an employee why their hours got cut because the franchisor changed the contract.
Physicians have done all three. You sign payroll. You absorb conversion factor cuts. You explain to staff why bonuses are smaller this year because a payer denied another batch of clean claims.
Hern is one of a handful of senators who would walk into Senate Finance with that scar tissue.
He starts the race with seven million dollars in cash. His senior advisor is Tony Fabrizio, the lead pollster for President Trump’s 2016 and 2024 campaigns. His early endorsements include Senators Bill Hagerty, Ron Johnson, Rick Scott, and Jim Banks.
The hospital lobby has already noticed.
THE RECEIPT
Hern’s most-cited healthcare bill is the CHOICE Act.
He introduced it. He passed it through Ways and Means on a 25-18 vote on June 7, 2023. The House passed it 220-209 on June 21, 2023.
The bill expanded individual coverage of Health Reimbursement Arrangements. It lets employers fund employees’ own coverage decisions instead of locking them into a corporate-managed plan. The Biden administration opposed it. Hern called the opposition “a badge of honor.”
The receipt that matters more for this election is older and quieter.
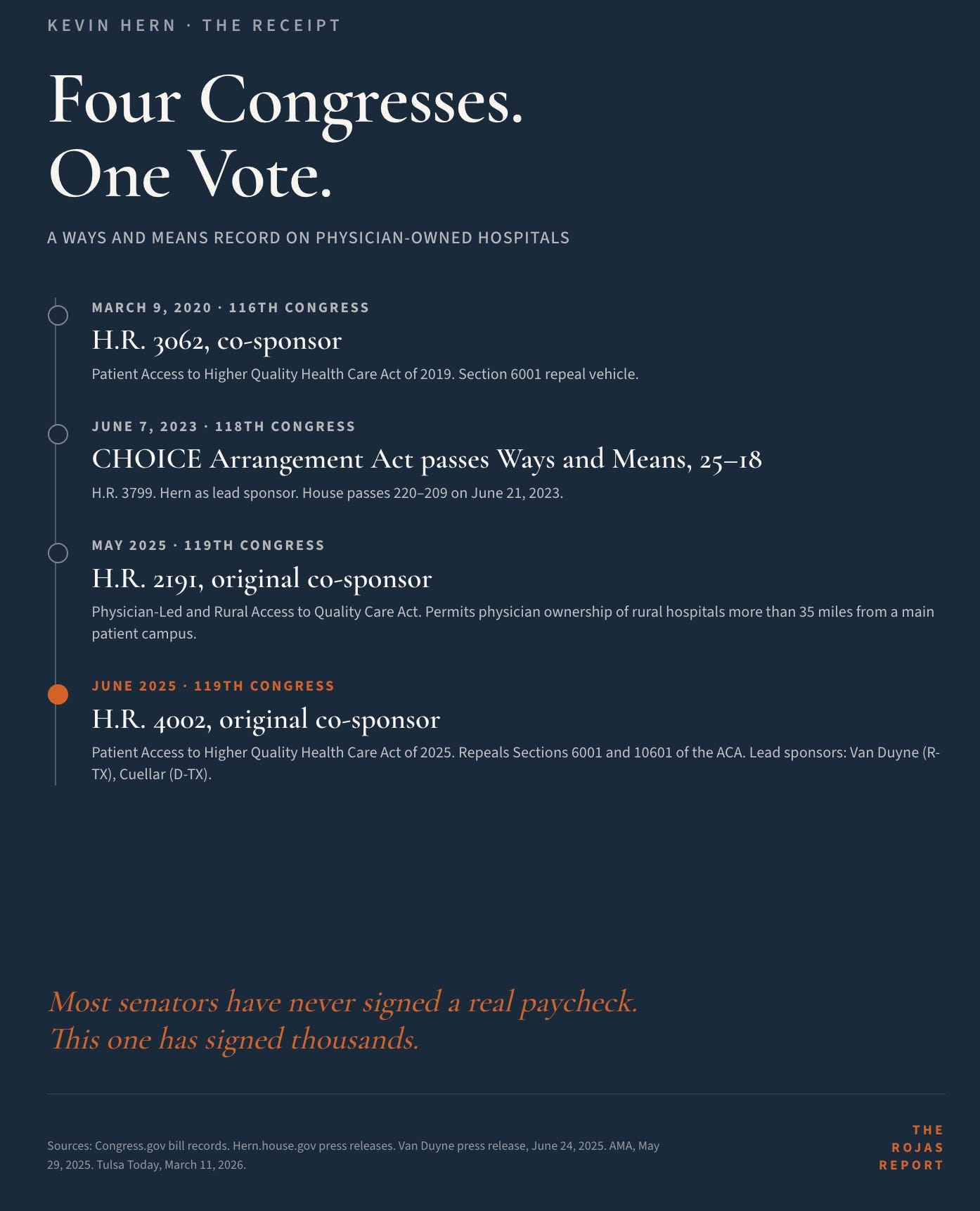
Hern is an original co-sponsor of H.R. 4002, the Patient Access to Higher Quality Health Care Act of 2025, introduced by Reps. Beth Van Duyne (R-TX) and Henry Cuellar (D-TX). The bill repeals Sections 6001 and 10601 of the Affordable Care Act, the provisions that froze new physician-owned hospitals out of Medicare in 2010 and capped existing facilities at their March 2010 bed and operating room counts.
His statement on introduction:
“We need innovation and competition in the healthcare space, and physician-owned hospitals often have high rates of patient satisfaction. Doctors spend the most time with patients; they ought to have the opportunity to own and operate their own hospitals. Let’s remove the barriers for those who are providing the actual care.”
He is also an original co-sponsor of H.R. 2191, the Physician-Led and Rural Access to Quality Care Act, introduced by Rep. Morgan Griffith (R-VA), which permits physician ownership of rural hospitals more than 35 miles from a main patient campus.
He signed on to the same vehicle as far back as the 116th Congress, when it was H.R. 3062 in 2019.
The receipts cover four congresses with three sponsors.
The commitment was consistent.
That matters in a Senate where most members have never met an independent physician.
The hospital lobby is counting on you not paying attention.
One hundred thousand physicians and healthcare operators refuse to comply. Read this newsletter at read.rojasreport.com.
THE LOBBY HE WILL HAVE TO BEAT
Three names defend the status quo.
Rick Pollack, American Hospital Association president. He has run AHA since 2015. He announced in December 2025 that he will retire by the end of 2026, but he is fully engaged through the transition, which means he is fully engaged through this election. AHA’s $29 million in 2024 federal lobbying does not include state association coordination, which adds further millions across the cycle. His job is to protect the hospital outpatient department reimbursement premium that lets a hospital collect 2.5 times the Medicare payment a physician’s office gets for the same service.
Charlene MacDonald, Federation of American Hospitals president and CEO since January 1, 2026. She replaced Chip Kahn, who retired after twenty-four years running FAH. Kahn is the legislative architect of Section 6001 of the ACA, the provision that froze the physician-owned hospital industry in 2010. MacDonald inherits that legacy and the budget that defends it.
David Skorton, Association of American Medical Colleges president and CEO since 2019. AAMC defends the academic medical center subsidy structure: graduate medical education funding, deep 340B participation across member teaching hospitals, and disproportionate share hospital payments. AMCs operate on a federal subsidy stack that community physicians cannot access. AAMC’s job is to keep that stack intact.
Three offices.
Three legislative agendas.
And every one of them has a budget that funds at least eight people whose only job is to remind senators which way to vote on physician payment.
You have the moral high ground.
They have a federal lobbying budget.

THE MATH
The federal individual contribution limit for the 2025-2026 cycle is $3,500 per election. A primary plus a general contribution combined is $7,000 maximum per individual. Couples giving jointly may contribute up to $14,000 combined for the cycle.
Now the cost of inaction.
Avalere studied how Medicare expenditures change when an independent physician transitions to a hospital-affiliated model. The study, commissioned by the American Independent Medical Practice Association in September 2024, analyzed five specialties: cardiology, gastroenterology, medical oncology, orthopedics, and urology.
Per beneficiary per year, when a physician moved from independent to hospital affiliation, total Medicare expenditures went up by a weighted average of $1,327. When they moved to a corporate affiliation, expenditures increased by $1,140.
Apply that to your panel. A physician treating 1,500 Medicare beneficiaries in an independent practice represents $1,327 multiplied by 1,500 in additional Medicare spending the moment that practice gets absorbed by a hospital system.
Two million dollars per practice. Per year. Permanent.
That is the consolidation cost.
Now, the related fight runs through the same committee. Site-neutral payment.
The Congressional Budget Office estimates that aligning Medicare payments for outpatient services commonly delivered in physician offices, hospital outpatient departments, and independent physician offices would save Medicare $157 billion over 10 years.
Site-neutral payment is the cleanest single committee fight in healthcare.
The Senate Finance Committee will run that fight between 2027 and 2030.
Hern starts his race with seven million dollars in cash. The hospital industry spent $116 million on federal lobbying in 2024 alone. The math against this seat is not a question of capability.
The math problem is not whether he can win. The math problem is whether independent medicine shows up before the primary deadline or after the loss.
The deals get cut before the press release.
Subscribe to Read.rojasreport.com and find out first.
THE REAL TAKEAWAY
This article is not really about Congressman Kevin Hern running for Senate.
Hern is the test case.
The article is about the thirty-year pattern that produced the fee schedule you currently work under. Hospitals treated federal political giving as a permanent operating expense. Physicians treated it as an occasional emotional reaction after another policy loss.
That is the entire difference.
Independent medicine does not need a single hero. It needs to learn that the hospital lobby is not winning because hospital arguments are better.
It is winning because hospital giving is permanent, disciplined, and structural, and physician giving is sporadic, reactive, and undercapitalized.
If physicians treated political giving the way hospitals do, the conversion factor would not look the way it does. The site-of-service rules would not look the way they look. Congress would have repealed Section 6001 years ago.
Hern is one Senate seat. One open committee assignment. One cheap entry point in a 2026 cycle that will not be cheaper in 2028, 2030, or 2032.
The deeper move is to stop treating federal political giving as something you do when you are angry, and start treating it as a line item on your overhead.
The hospital lobby figured this out in 1975.
You have a deadline.
THE ASK
This is the first federal candidate The Rojas Report has explicitly underwritten.
Not a recommendation.
A position.
Kevin Hern for U.S. Senate.
Donation page: Kevin Hern Support Page
Federal individual limits: $3,500 primary, $3,500 general, $7,000 combined maximum per individual. Couples giving jointly may contribute up to $14,000 for the cycle.
Editorial endorsement. Not coordinated with the campaign or any affiliated political committee. Sourced and reported independently.
Stop mistaking political abstinence for professional virtue.
The other side never did.
-Rojas out.
GLOSSARY
Senate Finance Committee: The U.S. Senate committee with jurisdiction over Medicare, Medicaid, federal tax policy, and federal health programs. Congress sets the Medicare conversion factor in statute through this committee. The single most consequential committee for physician income.
Medicare Physician Fee Schedule (MPFS): The annual federal rule that sets payment rates for physician services in Medicare. Updated each year through a “conversion factor” adjustment. CMS writes the rule administratively under statutory authority Congress shapes.
Ways and Means Committee: The U.S. House counterpart to Senate Finance. Has jurisdiction over Medicare and federal tax policy in the House. Hern’s current committee.
Section 6001 of the Affordable Care Act: The 2010 ACA provision that effectively banned new physician-owned hospitals from participating in Medicare and capped existing facilities at their 2010 bed and operating room counts.
H.R. 4002 (Patient Access to Higher Quality Health Care Act of 2025): The current vehicle to repeal Sections 6001 and 10601 of the ACA. Lead sponsors are Reps. Beth Van Duyne (R-TX) and Henry Cuellar (D-TX). Hern is an original co-sponsor.
H.R. 2191 (Physician-Led and Rural Access to Quality Care Act): A narrower vehicle that allows physician-owned hospitals more than 35 miles from a main patient campus or critical-access hospital. Hern is an original co-sponsor.
CHOICE Arrangement Act (H.R. 3799): Hern’s 2023 bill expanding individual coverage Health Reimbursement Arrangements. Passed the House 220-209 on June 21, 2023.
Site-of-Service / Site-Neutral Payment: Federal payment policy that produces different reimbursement rates for the same service depending on whether it is delivered in a hospital outpatient department, an ambulatory surgery center, or an independent physician office. Hospital outpatient rates are systematically higher.
340B: A federal drug pricing program created in 1992 to allow safety-net hospitals and clinics to purchase outpatient drugs at deeply discounted prices. Has expanded far beyond its original safety-net intent.
Avalere / AIMPA Study: The September 2024 whitepaper, “Medicare Service Use and Expenditures Across Physician Practice Affiliation Models,” commissioned by the American Independent Medical Practice Association. The current authoritative source on what happens to Medicare expenditures when independent physicians get absorbed into hospital and corporate models.
LDA (Lobbying Disclosure Act of 1995): The federal law requiring quarterly disclosure of lobbying activity. Source for all federal lobbying expenditure figures cited in this article.
SOURCES
The Hill, “Kevin Hern launches Senate bid for Markwayne Mullin’s Oklahoma seat,” March 11, 2026.
Tulsa Today, “Kevin Hern Announces for U.S. Senate,” March 11, 2026.
Oklahoma Voice, “Hern launches bid for US Senate, will not seek another term in House,” March 11, 2026.
Congress.gov, H.R. 3799, 118th Congress, CHOICE Arrangement Act.
House Ways and Means Committee, H.R. 3799 one-pager and Committee Report 118-107.
Hern.house.gov, “Hern bill passes Ways and Means Committee,” June 7, 2023.
Van Duyne press release, “Van Duyne Leads Bipartisan Legislation to Expand Patient Access to High Quality Health Care,” June 24, 2025.
AMA, “Bill introduced to allow physician-owned hospitals in rural areas,” May 29, 2025.
Hern.house.gov, “Rep. Hern signs on to bill allowing expansion of physician-owned hospitals,” March 9, 2020.
Avalere Health and AIMPA, “Medicare Service Use and Expenditures Across Physician Practice Affiliation Models,” September 2024.
OpenSecrets, “American Hospital Assn Lobbying Profile.” Source for AHA federal lobbying spend of $29,017,803 in 2024.
Taylor et al., “Patterns of Federal Lobbying by the Hospital Industry,” JAMA Health Forum, 2025.
Bipartisan Policy Center, “Site Neutrality in Medicare Payment,” updated December 2025.
KFF, “Five Things to Know About Medicare Site-Neutral Payment Reforms,” August 2025.
AHA press release, “American Hospital Association President and CEO Rick Pollack Announces Retirement,” December 10, 2025.
FAH press release, “After Nearly a Quarter Century of Leadership, Chip Kahn to Retire from the Federation of American Hospitals,” June 6, 2025.
Chief Healthcare Executive, “Federation of American Hospitals names new CEO with policy expertise.”
AAMC, “David J. Skorton, MD” leadership biography.
Federal Election Commission, “Contribution limits for 2025-2026,” published January 30, 2025.
Donated! Thanks Dutch.