
Healthcare 2025: The Year We Stopped Pretending

Tonight, 22 million Americans lose their health insurance subsidies.
Tomorrow, they find out the ACA never actually helped them.
That’s not a policy change.
That’s a confession.

What We’re Covering Today.
COVID subsidies expire tonight and what it reveals about the ACA
Congress pays hospitals 145% more than independent physicians for the same work
The Thompson assassination and the nonprofit hospitals doing the same thing
GLP-1s are reversing chronic disease and threatening the business model
$18 billion in Medicaid fraud under Tim Walz that nobody wants to discuss
RFK Jr. talks fluoride while CMS runs Soviet-style central planning
How the One Big Beautiful Bill actually had to pass
PBM reform has bipartisan support and zero action
The donation economy that keeps healthcare broken
2026: The Rojas Report agenda
New to healthcare policy? Definitions are at the bottom.
1. COVID Subsidies Die Tonight
Tonight, 22 million Americans lose their health insurance subsidies. Tomorrow, they find out the ACA never actually helped them.
The enhanced premium tax credits were pandemic emergency relief. Extended through the Inflation Reduction Act. Always set to expire December 31, 2025.
Congress chose not to extend. A 42-day shutdown. Political theater. No plan.
Here’s what nobody will say: premiums aren’t doubling. They’re returning to where they always were.
If “expiration” means doubling, then the ACA never actually made coverage affordable. The subsidies masked the failure.
22 million people received temporary relief from a system that never fixed underlying costs.
And why is the federal government handing $40 billion to insurance companies as subsidies for copays and deductibles? These are Cost Sharing Reduction payments. They go directly to insurers. Not to patients. To carriers.
The money flows to insurers. The prices stay high. The patient stays stuck.
The ACA didn’t solve anything. It laundered taxpayer dollars through the insurance industry.
2. Congress Hates Doctors, Including the Doctors in Congress
Some doctors in Congress have an F on healthcare. They campaign in white coats and vote with the hospital lobby.
Every piece of legislation makes independent practice harder:
MACRA/MIPS reporting burdens
Prior auth requirements
Fee schedule cuts
Scope creep eroding physician authority
Corporate practice of medicine workarounds
And here’s the number that should make your blood boil:
CMS pays hospitals 145% more than independent physicians for the same work.
Same CPT code. Same service. Same patient. The hospital gets paid nearly 2.5x.
That’s not an accident. That’s policy. That’s the fee schedule protecting consolidated systems while crushing independent practice.
Physician-legislators campaign on their credentials. Then they vote for every hospital lobby priority that crosses their desk.
Some of those doctors have an F on the scorecards.
The Rojas Report will expose them in 2026. Names. Votes. Grades. Public.
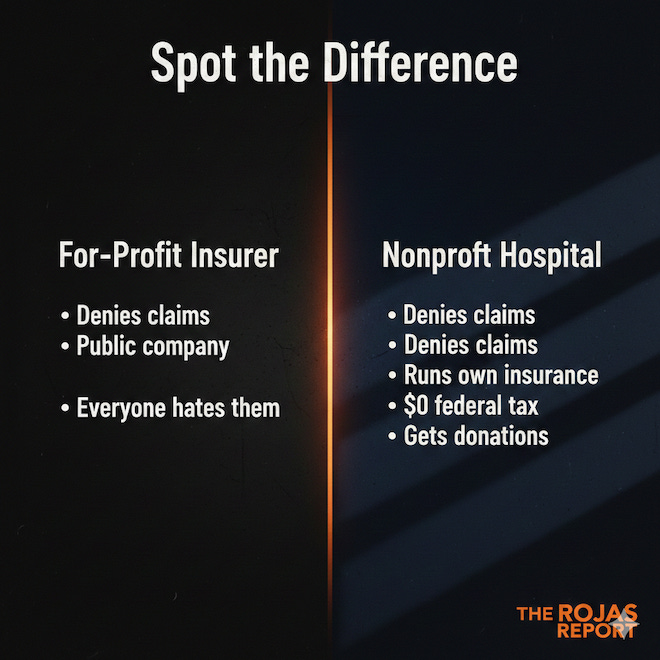
3. The Thompson Assassination: Misdirected Rage
Why do Americans rage at insurance companies but write checks to the nonprofit hospitals doing the same thing?
Murder is wrong. Full stop.
Now, let’s talk about where that anger went and where it didn’t. Brian Thompson ran UnitedHealthcare.
Public company.
Shareholder accountability.
Everyone knows to hate them.
Meanwhile, your local nonprofit health system:
Runs its own insurance company
Denies claims
Sends patients to collections
Pays executives $5-10 million annually
Pays zero federal income tax
Your favorite college football team’s hospital screws you over and puts you into collections. And you write them a donation check anyway.
UnitedHealthcare is the visible villain.
The Five Dynasties of nonprofit healthcare laundered their reputation with children’s hospitals, naming rights, and community benefit statements that mean nothing.
The target selection revealed how successfully the nonprofit hospital lobby has stayed invisible.
The rage is legitimate. The aim was off.
Most people sacrifice. They accept good enough because finding the best is exhausting. You’re not most people. You’re here because you want to understand how the system actually works. The Rojas Report is for the 3% who refuse to be played.
4. GLP-1s: The Thing That’s Actually Working
15-25% sustained weight loss. Cardiovascular risk is dropping. Inflammation declining. Joint replacements are falling. One drug class is doing what public health couldn’t do in 50 years.
Ozempic. Wegovy. Mounjaro. Zepbound.
These drugs are doing what decades of campaigns, programs, and initiatives couldn’t: actually reversing metabolic disease at scale.
Here’s what’s happening downstream:
Knee and hip replacements are declining. When people lose 50-80 pounds, mechanical stress on joints drops. Orthopedic surgeons are watching volumes soften.
Grocery spend is down. People on GLP-1s eat less. Walmart, Nestlé, and others have publicly acknowledged the impact.
Inflammation and chronic disease markers are declining. Diabetes management is improving. A1C levels are dropping. Cardiovascular risk markers are improving.
The chronic disease cascade is being interrupted at the front end.
Now ask yourself: Who loses when chronic disease declines?
Hospital systems: fewer admissions, fewer complications
Dialysis companies: slower pipeline
Food industry: lower consumption
GLP-1s are the first real threat to the business model built on managing chronic disease rather than reversing it.
The system profits from sickness. These drugs expose the misalignment.
5. The Medicaid “Cuts” Narrative vs. $18 Billion Minnesota Fraud
They called work requirements “cruel.” They ignored $18 billion stolen from the poorest Americans.
The same voices screaming about Medicaid cuts in the One Big Beautiful Bill conveniently ignored the largest Medicaid fraud in American history.
Tim Walz was the governor of Minnesota. $9 billion confirmed stolen, with an estimated $18 billion when the dust settles.
Feeding Our Future. Millions siphoned through fake childcare and meal programs. Money meant for vulnerable populations.
Where was the outrage? Where were the progressive healthcare advocates demanding accountability?
A single whistleblower found it. Not CMS. Not a federal audit. Not oversight. An accident.
You can’t call Medicaid sacred while letting $18 billion walk out the door. Stewardship matters.
Work requirements and eligibility verification aren’t cruel.
They’re basic governance that Minnesota apparently forgot existed.
The fraud story has chapters in every state.
Minnesota is just the biggest…for now.
6. RFK Jr.: MAHA Theater While CMS Burns Down the House
CMS runs Soviet-style central planning invented in 1921. Every insurer follows its lead. Kennedy talks about fluoride. The fee schedule stays untouched.
Secretary Kennedy gave the MAHA crowd their wins:
Fired ACIP members
Changed vaccine schedules
Talked about seed oils and fluoride
Investigated autism causes
He even recommended a second COVID booster for older people against the wishes of team MAHA and still the vax everyone crowd complains.
But here’s what he hasn’t touched:
CMS fee schedules. The Medicare Physician Fee Schedule uses Soviet-era methodology. Command-economy central planning. Every private insurer benchmarks its rates against Medicare rates.
Site-neutral payments. Hospitals get paid 145% more than independent physicians for identical services. That differential drives consolidation, destroys independent practice, and inflates every premium in America.
Kennedy talks about what’s in food.
CMS controls what healthcare costs.
Fee schedules control healthcare premiums!
Problem solved tomorrow.
If you’re a consultant selling “site-neutral bad, nonprofit hospital good,” you’re getting paid right now.
Everyone else is getting played.
7. How Laws Actually Get Made
Reconciliation. Byrd Rule. 51 votes. Tax cuts expiring. Debt ceiling. Medicaid offsets. That’s not evil. That’s the only vehicle that moves. The question is what was never on the table.
Everyone screamed about the One Big Beautiful Bill. Almost no one understood how it had to pass.
Reconciliation is a budget tool. One shot per fiscal year. Bypasses the filibuster. Requires a simple majority. Must focus on revenue and spending under Byrd Rule constraints.
The OBBBA wasn’t some evil plot. It was the only legislative vehicle that could move.
Tax cuts were expiring. The debt ceiling needed addressing. Medicaid “cuts” got packaged as offsets because that’s how reconciliation math works.
The outrage machine screamed “they’re gutting healthcare!” without understanding the mechanics.
The real question nobody asks: Why is Medicaid the offset every single time?
Because touching nonprofit hospital tax exemptions would require 60 votes. Addressing the $150 billion in structural advantages would require actual bipartisan will. Federal incentives to repeal state CON laws? Never even discussed.
Those are protected. Medicaid eligibility is not.
The priorities are exposed not by what passed, but by what was never on the table.
8. PBM Reform: Bipartisan Agreement, Zero Action
PBM reform is a rare bipartisan issue. The fact that nothing’s happened tells you exactly how power works.
Pharmacy Benefit Managers operate the most opaque toll booth in American healthcare:
Spread pricing
Rebate retention
Vertical integration with insurers and pharmacies
DIR fees are crushing independent pharmacies
The FTC has been investigating. Congress holds hearings. States pass laws.
CVS Caremark, Aetna, UnitedHealth, Optum, Express Scripts, and Cigna keep printing money.
Three companies control 80% of the market. Everyone agrees it’s broken.
Nothing changes.
Left and right agree PBMs are a problem. The PBMs keep winning anyway.
That tells you everything about how power actually works in healthcare. The PBMs have bought enough protection to survive every news cycle.
This has to break eventually. The question is whether it breaks through legislation or through the system collapsing under its own contradictions.
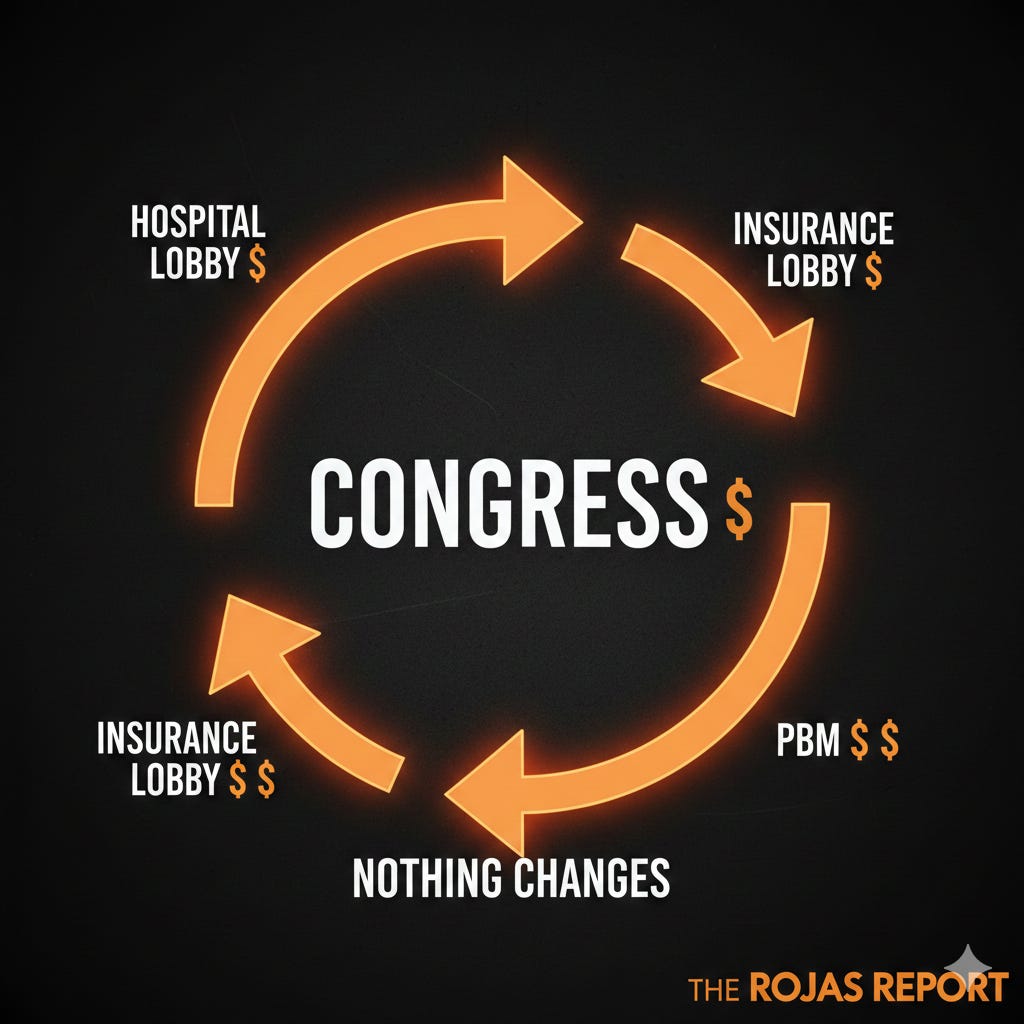
9. The Donation Economy
Politicians collect from hospitals, insurers, pharma, and PBMs, then do nothing. That’s not incompetence. That’s the business model.
Why would Congress fix healthcare premiums when the crisis is the fundraising engine?
Every election cycle:
“Healthcare costs are out of control!”
“We have to protect coverage!”
“The other side wants to take away your insurance!”
The emails go out. The donations roll in. The problem persists.
Solved problems don’t raise money.
A congressman who actually fixes premium costs loses the issue. No more mailers. No more town halls about the crisis. No more PAC dollars from stakeholders who need a seat at the table.
The hospital lobby donates to keep their tax exemptions and CON protections.
The insurance lobby donates to keep its regulatory moat.
Pharma donates to protect pricing.
PBMs donate to stay opaque.
Politicians collect from all sides. Fix nothing. Keep the fundraising engine running.
Donations stop when problems stop. That’s why issues don’t stop.
10. Priorities in 2026: The Rojas Report Agenda
Scorecards. Premium accountability. CMS education.
Five Dynasties exposed. Fraud documentation. Midterm framing.
One publication. One agenda.
The midterms will be about Medicaid fraud and health insurance premiums. The American public will understand that it all begins with CMS fee schedules and flows to commercial from there.
United Healthcare does nothing without CMS’s permission.
Neither does any other commercial insurer.
Here’s what The Rojas Report delivers in 2026:
Scorecards:
Grading every healthcare vote. Exposing captured physician-legislators. Names. Votes. Grades. Public.
Premium Accountability:
Connecting voter premiums to specific systems, specific CON laws, specific votes. Make it local. Make it named.
CMS Education:
Making fee schedule mechanics understandable so Americans see where pricing starts.
Five Dynasties Continuation:
Naming the nonprofit systems. Executive comp. Tax advantages. Collection practices. Community benefit that isn’t.
Fraud Accountability:
Minnesota is chapter one. Every state has a story.
Midterm Framing
Medicaid fraud plus premium crisis equals the kitchen table issue.
The Framework
Healthcare isn’t broken. It’s rigged.
Every story in 2025 confirms it. The protected stay protected. The vulnerable get cut. The rage gets misdirected. The theater distracts from the structure. The one thing working threatens the business model. And the donation economy ensures nothing changes.
And we’re still paying taxes? For what? More irresponsible oversight?
Minnesota’s $18 billion fraud was found by accident. A single whistleblower. Not an audit. Not a federal review. Not CMS. An accident.
Imagine what happens when we actually start looking.
The truth is, one-third of this country is on the take. Hospital executives. Administrators. Consultants. Lobbyists. Politicians. Staffers. The entire apparatus that sits between a doctor and a patient, extracting tolls and adding zero value.
They don’t want us looking. That’s why the system stays opaque. That’s why the fee schedules are incomprehensible. That’s why CON laws remain on the books. That’s why nonprofit financials are buried. That’s why fraud takes a decade to surface.
2026 is the year we name names. We start looking. And we don’t stop.
You’ve read 3,000 words that no health system or insurance carrier PR team wants you to see. That took time to research. It takes independence to publish. We love readers who’d rather understand the system than be played by it. If that’s you, subscribe.
Follow
X: @dutchrojas
YouTube: @dutchrojas
LinkedIn: linkedin.com/in/dutchrojas
How to Work with Dutch
Independent physicians → MedMerge (CEO). Reduce P&C, benefits, retirement, and payroll costs through cooperative scale. Move liabilities to assets.
Healthcare startups → PhyCap Fund (General Partner). Investment and strategic guidance.
Employers → Health plan review. You’re probably overpaying by 30-50%.
Podcasts/stages → Booking available.
Legislators/staffers → Data briefings on healthcare economics.
Glossary
ACA — Affordable Care Act. The 2010 healthcare law. Enhanced premium tax credits added during COVID expire tonight.
CMS — Centers for Medicare & Medicaid Services. The federal agency that sets Medicare payment rates. Every private insurer benchmarks off CMS.
CON Laws — Certificate of Need laws. State regulations require government approval before building new healthcare facilities. Protects incumbents from competition.
Cost Sharing Reduction (CSR) — Federal payments to insurers to reduce copays and deductibles for low-income ACA enrollees. $40 billion annually going directly to carriers.
CPT Code — Current Procedural Terminology. Standardized codes for medical services. Same code, different payment depending on the setting.
Five Families — The Rojas Report framework for the five largest commercial insurance companies.
Five Dynasties — The Rojas Report framework for the largest nonprofit health systems operating with tax exemptions, monopoly pricing, and regulatory capture.
GLP-1 — Glucagon-like peptide-1 receptor agonists. Drug class including Ozempic, Wegovy, Mounjaro, and Zepbound. Treating obesity and diabetes with unprecedented efficacy.
MACRA/MIPS — Medicare Access and CHIP Reauthorization Act / Merit-based Incentive Payment System. Federal quality reporting requirements adding administrative burden to physicians.
OBBBA — One Big Beautiful Bill Act. The 2025 budget reconciliation law signed July 4, cutting approximately $1 trillion from Medicaid.
PBM — Pharmacy Benefit Manager. Intermediaries controlling drug pricing and formularies. Three companies control 80% of the market.
Site-Neutral Payment — Policy requiring equal payment for the same services regardless of setting. Currently, hospitals receive 145% more than independent physicians.
© 2025 The Rojas Report. All rights reserved.
Healthcare isn’t broken. It’s rigged. We have the receipts.
-Rojas out
Almost everything you wrote makes 100% sense. Thank you and Happy New Year. Looking forward to your 2026 production.
Just two quibble items for you today.
1. Tiny quibble:
- The $18 billion graphic has two typos.
- The Spot the Difference has “Denies claims” listed twice in the right column (maybe intentional?).
2. Bigger quibble: 4. GLP-1s: The Thing That’s Actually Working.
GLP-1s may be false prophets (profits). Please consider this article by A Midwestern Doctor (summarized in a Substack Note):
Unmasking The Great Ozempic Scam. The GLP-1 saga epitomizes the unsustainable corruption within our medical system. By A Midwestern Doctor (12/28/25). https://tinyurl.com/33prt3uw
The time and effort that you take to research and report on these issues must be enormous and deserves widespread recognition and appreciation. Can't wait for the whole series. I am especially interested in hearing about the politicians that are the worst offenders (as I am certain they all participate to some degree.)