Healthcare Didn’t Capture Congress. Congress Handed Healthcare the Keys in 1980.

The hospital industry’s entire lobbying architecture was described publicly by a Nobel laureate on daytime television before most physicians practicing today were born. The AHA took notes. Nobody handed the notes to the physicians.
Twelve principles. One broadcast. Forty-five years.
In one hour on Phil Donahue in March 1980, Milton Friedman named every regulatory capture mechanism the American hospital industry would spend the next four and a half decades weaponizing.
The broadcast is public record. The playbook is open. The prosecution starts below.
IN TODAY’S ARTICLE:
Twelve regulatory capture principles from one 1980 broadcast, each with a healthcare receipt
The $6 billion pharmaceutical-to-advocacy funding flow that launders industry lobbying as patient advocacy
The 22-percent airline fare reduction that proves deregulation broadens ownership instead of narrowing it
The 88%/12% dependency structure that explains every dollar the AHA spends keeping physicians employed, distracted, and atomized
Glossary at the bottom of today’s article.
A note on what follows…
That afternoon’s featured book was Free to Choose. Adam Smith sat on the cover. The audience was suburban housewives in Chicago.
Milton Friedman did not say the word “healthcare” once in the entire hour.
He described, in complete detail, the regulatory mechanisms the American Hospital Association, the Federation of American Hospitals, and the American Medical Association spent the next 45 years weaponizing into the most extractive medical-industrial complex in human history.
The Interstate Commerce Commission as a template for regulatory capture. Incumbents writing their own rules. Subsidies disguised as public protection. “Affecting to trade for the public good” while the public pays the bill.
The hospital industry watched the broadcast and recognized a playbook.
The physicians watched the broadcast and heard an economics lecture.
Only one of those groups was paying attention.
What follows are twelve principles Friedman articulated that afternoon, and the receipts for what each one became in American medicine by 2026.
1. “Affecting to trade for the public good” is the entire hospital lobbying script.
Friedman quoted Adam Smith on air: nobody lobbies Congress saying “pay me a bonanza.” They lobby saying the public will be harmed if you do not.
Every piece of hospital industry testimony before Ways and Means, Energy and Commerce. Senate HELP, and Finance follows this template exactly.
340B expansion testimony claims safety-net protection. The receipt shows that 340B hospitals collect commercial spreads on drugs dispensed to insured patients in wealthier zip codes than the hospitals’ own patient catchment areas.
Site-neutral opposition claims rural hospital protection. Rural hospital closures accelerated through the decade the AHA blocked site-neutral. The regulatory moat did not save rural hospitals. It protected urban HOPD margins.
CON law claims prevention of wasteful duplication. CON states have fewer ASCs per capita, higher hospital prices, and worse access to outpatient care than states that repealed.
The public-good frame is the sales pitch. The receipt is the tax return.
Rep. Greg Murphy (R-NC), a physician, sits on the Ways and Means Health Subcommittee. In the 2024 cycle, he accepted $68,000 from the Hospitals & Nursing Homes sector alone, including $12,500 from the Federation of American Hospitals PAC, while voting on Medicare physician payment rates. The committee that sets physicians’ earnings is funded by the entities that benefit when physicians earn less.
Smith described this in 1776. Friedman described it in 1980. The AHA executed it in 2026.
2. The ICC is the Rosetta Stone for healthcare regulation.
Friedman spent eight minutes on the Interstate Commerce Commission. The structure he described:
Reformers in the 1880s built the ICC to stop railroad monopoly abuse. The railroads captured the ICC within a decade. By the 1930s, the ICC existed primarily to block trucking competition on behalf of railroads. By 1980, a federal agency administered a trucking cartel.
The do-gooders moved on to the next cause. The incumbents took over the agency that was meant to restrain them. The public paid.
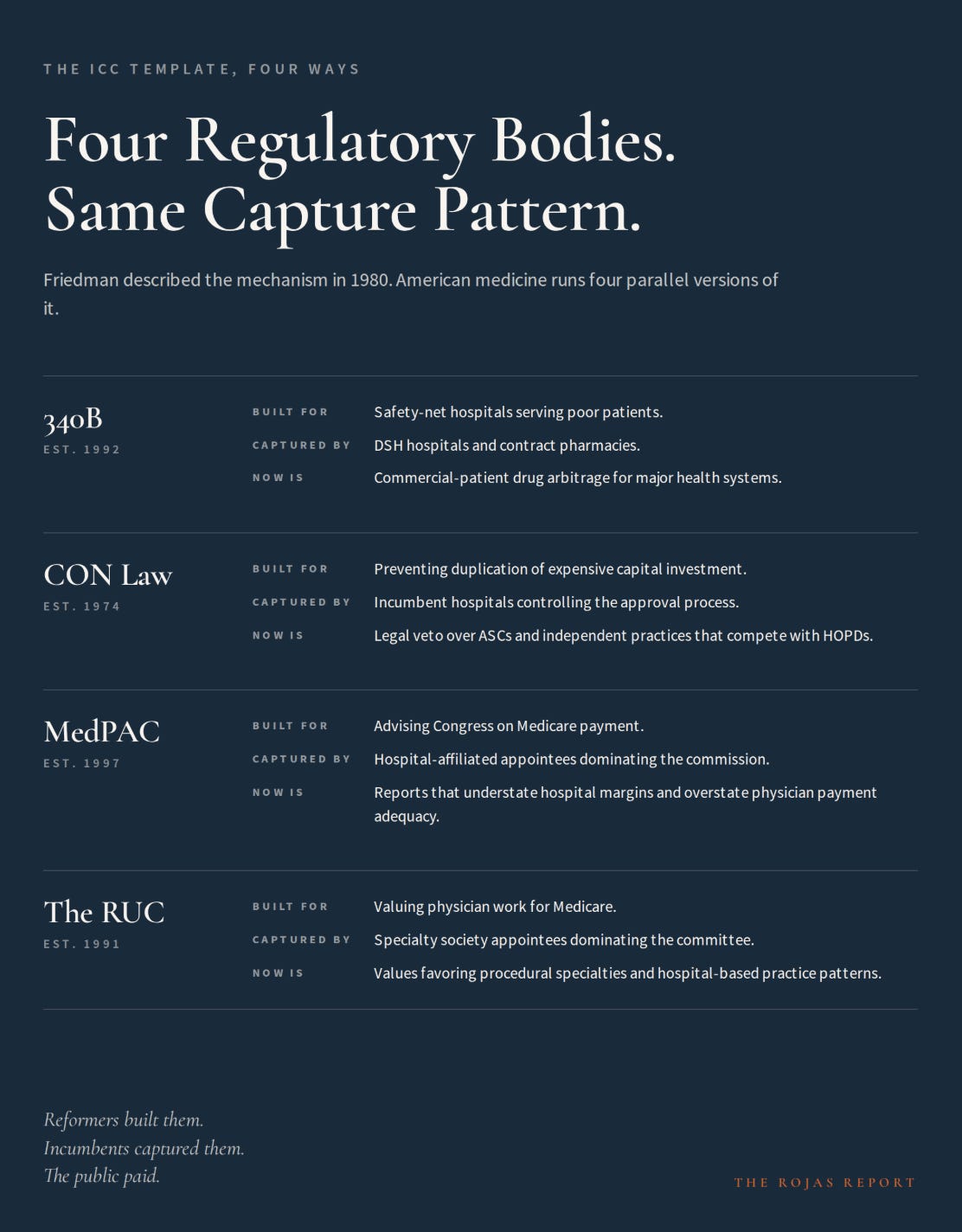
Healthcare runs four parallel versions.
340B (1992): Created to support safety-net hospitals serving poor patients. Over time, DSH hospitals and contract pharmacies took over the program. It now functions as a commercial-patient arbitrage generating billions in profit for major health systems with no requirement to serve the patients it was built for.
Certificate of Need (1974): The law aimed to prevent costly duplication. Incumbent hospitals took over approvals. Now, it acts as a legal veto over hospitals, ASCs, imaging centers, and independent practices competing with hospital outpatient departments.
MedPAC: The commission was built to advise Congress on Medicare payment. Hospital-affiliated appointees now dominate. As a result, reports understate hospital margins and overstate physician payment adequacy.
The RUC: Formed to value physician work. Now, specialty society appointees dominate. They set values favoring procedural and hospital-based practices.
Friedman described the mechanism. Four regulatory bodies demonstrate it.