
Hospital Outpatient Pay Rose 26% in a Decade. Physician Pay Fell 10%. Here's Who Engineered That.
The broken system narrative is the cover story. Once you see the architecture underneath it, you can't unsee it.

Everyone keeps asking why the system is broken.
Wrong question.
The system works exactly as designed.
The problem is who designed it and what it was designed to do.
IN TODAY’S ARTICLE:
The five families and five dynasties: who the system was actually built to serve
Citizens United, January 2010, and the $525 million in health sector lobbying that bought the ACA ten months later
How banking consolidation from 22,000 institutions to 6,000 became the blueprint for hospital consolidation
What “legibility” means, why administrative states need it, and why independent medicine is the enemy of it
Glossary at the bottom of today’s article.
Watch the full Vital Discourse episode on YouTube.
THE FIVE FAMILIES. THE FIVE DYNASTIES.
I was on Vital Discourse with Dr. Lee Mandel and Dr. Ben Cilento.
Two physicians who have spent their careers inside the system.
Smart guys. They ask the hard questions. We went long.
I want to capture the core of what we talked about, because it’s the same conversation I have in every doctor’s lounge, at every ASC conference, in every back hallway where physicians are actually honest with each other.
Let’s skip the sugarcoating:
Healthcare is not broken.
It was built this way.
The system has ten masters. Five families, five dynasties. The families are the insurance carriers. The dynasties are the nonprofit health systems, including the academic medical centers. Below them: PhRMA, AdvaMed, and AHIP, the trade lobby for insurance. These ten groups are those the system was designed to serve.
Supporting all of them, largely and unfortunately, is CMS.
The Centers for Medicare and Medicaid.
The people hurt by this design: every physician in independent practice, every patient who can’t afford their premium, and every nurse and clinician who chose medicine for the right reasons and is now drowning in prior authorizations.
The system doesn’t fail them.
It was built against them.
THE NUMBERS THAT EXPLAIN EVERYTHING
The Outpatient Prospective Payment System, the federal mechanism that created standardized facility fees for hospital outpatient services, took effect in August 2000. Before that, there was no uniform facility fee billing structure for outpatient care. The OPPS is where the divergence begins.
Here is what happened after that.
From 2000 to 2024, cumulative updates to the Medicare physician fee schedule totaled approximately 14%. Over that same period, the Medicare Economic Index, which measures the actual cost of running a physician practice, rose 56%.
That is not a gap.
That is a slow suffocation.
In inflation-adjusted terms, physician purchasing power fell by roughly 30 cents on every dollar over 24 years.
The hospital side ran in the opposite direction. Since 2016 alone, the hospital’s inpatient base rate has risen by 30%. The hospital outpatient base rate rose 26%. Physician rates fell 10% over that same decade.
In 2025, CMS cut physician reimbursement 2.9% and raised hospital outpatient reimbursement 2.9%. Same year. Mirror image. Not a coincidence.
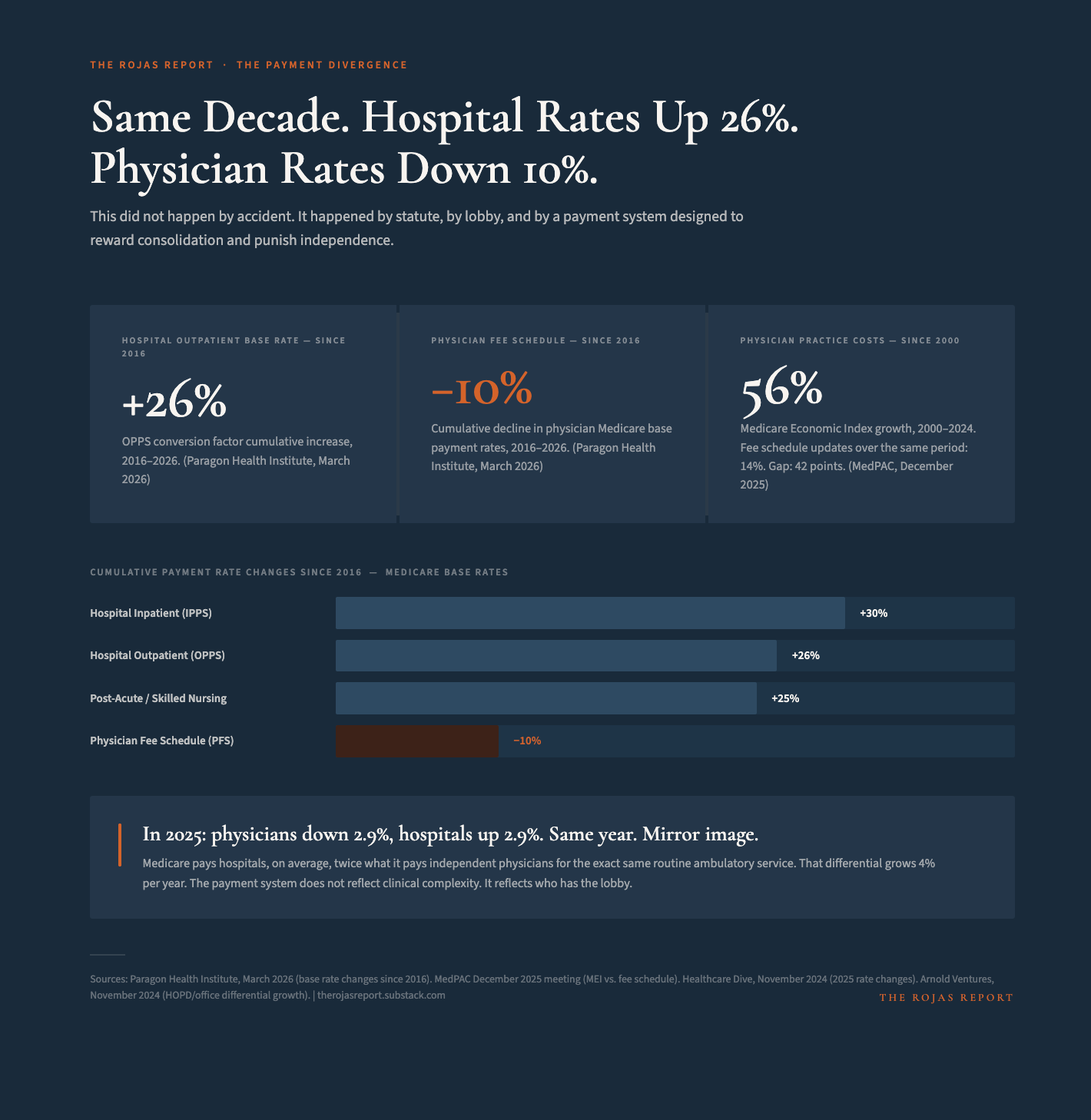
The divergence in payment rates is now so wide that Medicare pays hospitals, on average, twice what it pays independent physicians for the exact same service. For identical procedures. Same patients. Same clinical complexity. The only variable is who owns the building.
Blue Cross Blue Shield tracked the commercial side from 2017 to 2022. Hospital outpatient department prices grew 27% over five years. Physician office prices grew 2%. The gap between the two settings compounds every year.
This is not a coincidence. It is the result of deliberate lobbying. Health systems, particularly academic centers, deployed their lobbyists to expand eligibility for facility fees. They pushed for hospital outpatient department (HOPD) designation, which allows a physician’s office acquired by a health system to bill at hospital rates without any change in physical location, staffing, or overhead.
UPMC pushed hard on this.
Worked with their lobbyists.
Paid them millions.
Got it through.
Now, a health system can buy an ophthalmology practice in Pittsburgh and collect facility fees two hours from the main campus. The practice hasn’t moved. The care hasn’t changed. The bill has.
When a health system CEO buys every independent practice within a 60-mile radius, the break-even point for that acquisition is less than 18 months. Not because of clinical efficiency. Because of facility fee arbitrage, independent physicians cannot access.
I’ve seen it in South Florida. One academic center collecting 625% of Medicare. Jackson Baptist is just north of 300%. Independent physicians at 175-180%. Same procedures. Same patients. Same city.
The 80/20 rule in healthcare billing: facility fees dominate. The physician’s share is what remains.
A total joint replacement. The hospital collects $21,000 to $25,000. The surgeon who spent 45 minutes on your knee gets $1,200.
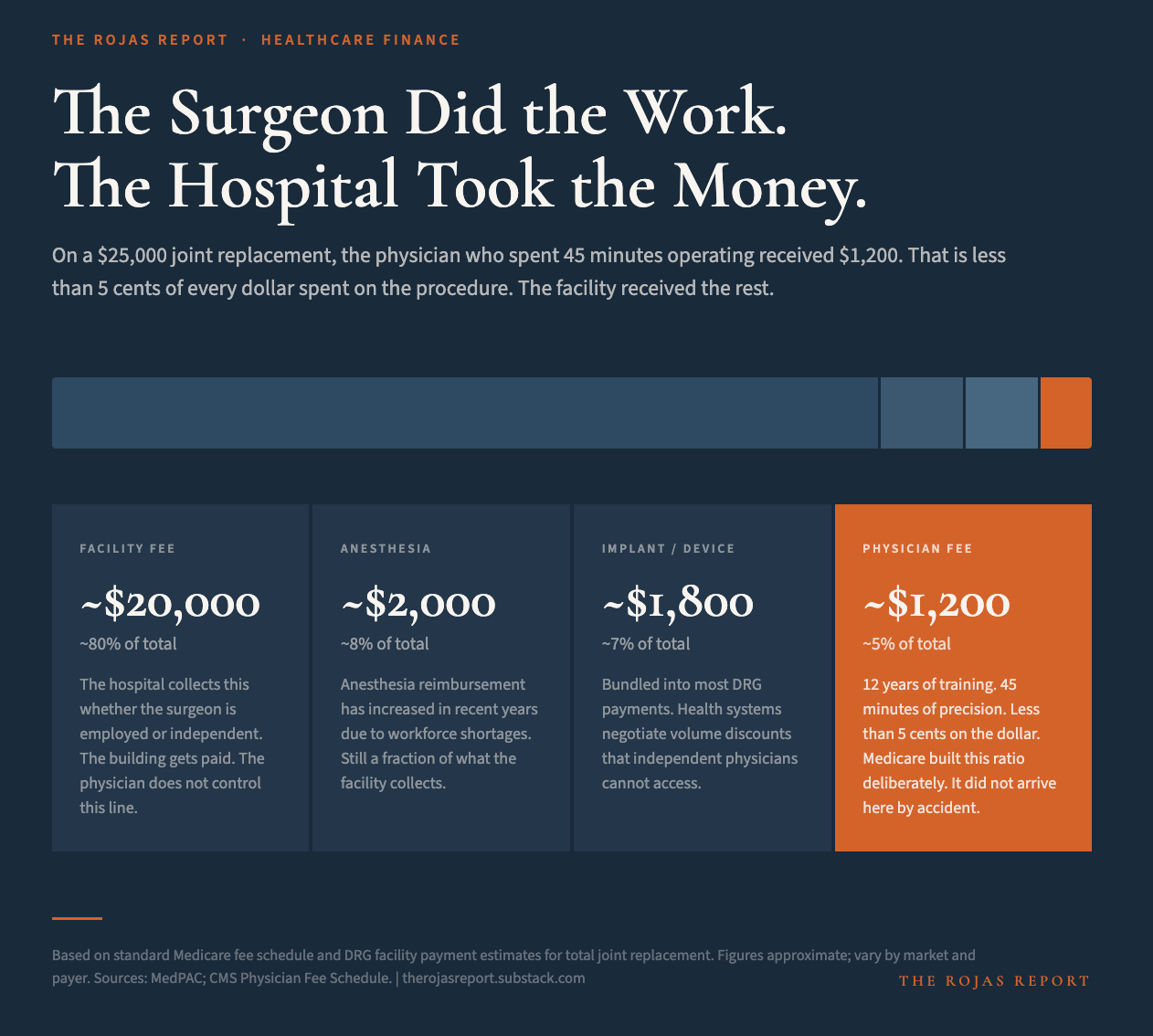
The cartel built a payment system that pays the building twice what it pays the doctor. You just read how it works.
What comes next is who built it, how they keep it funded, and what it does to a real patient in a real exam room.
