
Hospital Systems Don't Recruit Physicians. Congress Does.
Stark Law made it illegal for independent physicians to operate integrated practices. The employment exception made it legal for hospital systems to hire them. The recruitment pitch writes itself.

Everyone thinks Stark Law prevents corruption.
It does not.
It prevents independent physicians from operating integrated clinical delivery models. Hospital-employed physicians face no such constraint. The law does not ban self-referral. It bans self-referral by the wrong kind of physician.
IN TODAY’S ARTICLE:
How Stark Law criminalizes physician ownership of ancillary services while exempting hospital employment
The specific statutory language (42 USC 1395nn(a)(1) and (e)(2)) that creates a two-tier referral system
Why the lowest-friction path to integrated care runs through a hospital W-2
Thirty years of practice acquisitions walked on this conveyor belt
Glossary at the bottom of today’s article.
The Law That Built the Conveyor Belt
In 1989, Congress passed the physician self-referral prohibition, codified at 42 USC 1395nn and named after its primary sponsor, Representative Pete Stark. The stated purpose was straightforward: stop physicians from referring Medicare patients to entities in which the physician or an immediate family member holds a financial interest.
Fair enough on its face.
The logic went like this. A physician who owns a share of an MRI center has a financial incentive to refer patients to that center, regardless of medical necessity. Congress looked at that incentive and called it a problem.
So Congress built a wall.
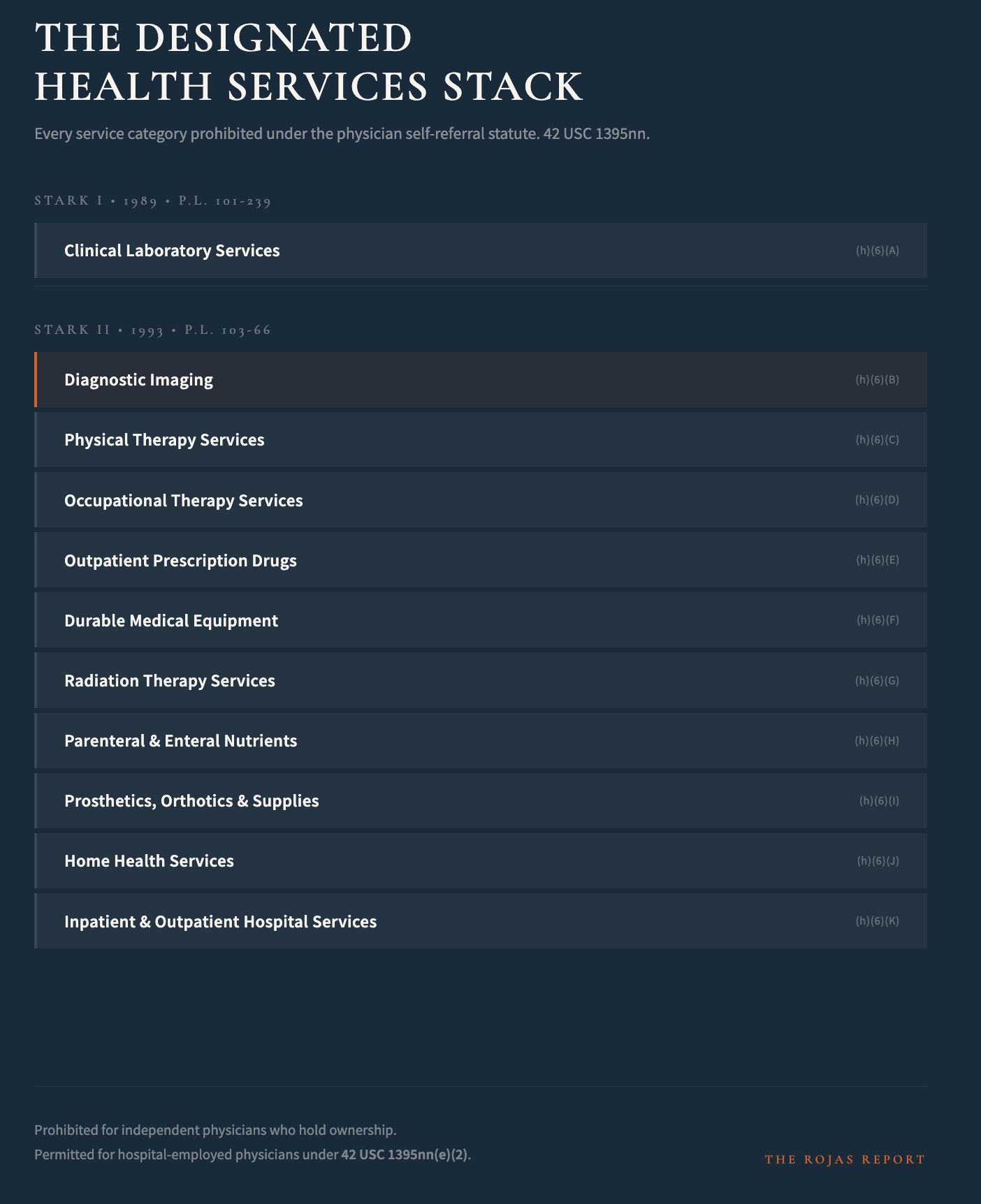
Stark I, enacted in the Omnibus Budget Reconciliation Act of 1989 (Public Law 101-239, Section 6204), applied the self-referral prohibition to clinical laboratory services. One service line. One prohibition. A targeted intervention.
Then came Stark II.
Four years later, the Omnibus Budget Reconciliation Act of 1993 (Public Law 103-66, Section 13562) expanded the prohibition to the full list of designated health services as defined at 42 USC 1395nn(h)(6). That list is not short.
Diagnostic imaging. Physical therapy. Occupational therapy. Outpatient prescription drugs. Durable medical equipment. Radiation therapy. Parenteral and enteral nutrients. Prosthetics, orthotics, and supplies. Home health services. Inpatient and outpatient hospital services.
The entire clinical ancillary stack.
After 1993, a physician with a financial interest in any entity providing any of those services could not refer a Medicare patient to that entity. Period. Unless a statutory or regulatory exception applied.
Congress did not build a guardrail. Congress built a cage. And then Congress handed the key to one class of physician while locking another class inside.
More physicians read The Rojas Report than their hospital system’s internal newsletter. There’s a reason for that. Subscribe.
