
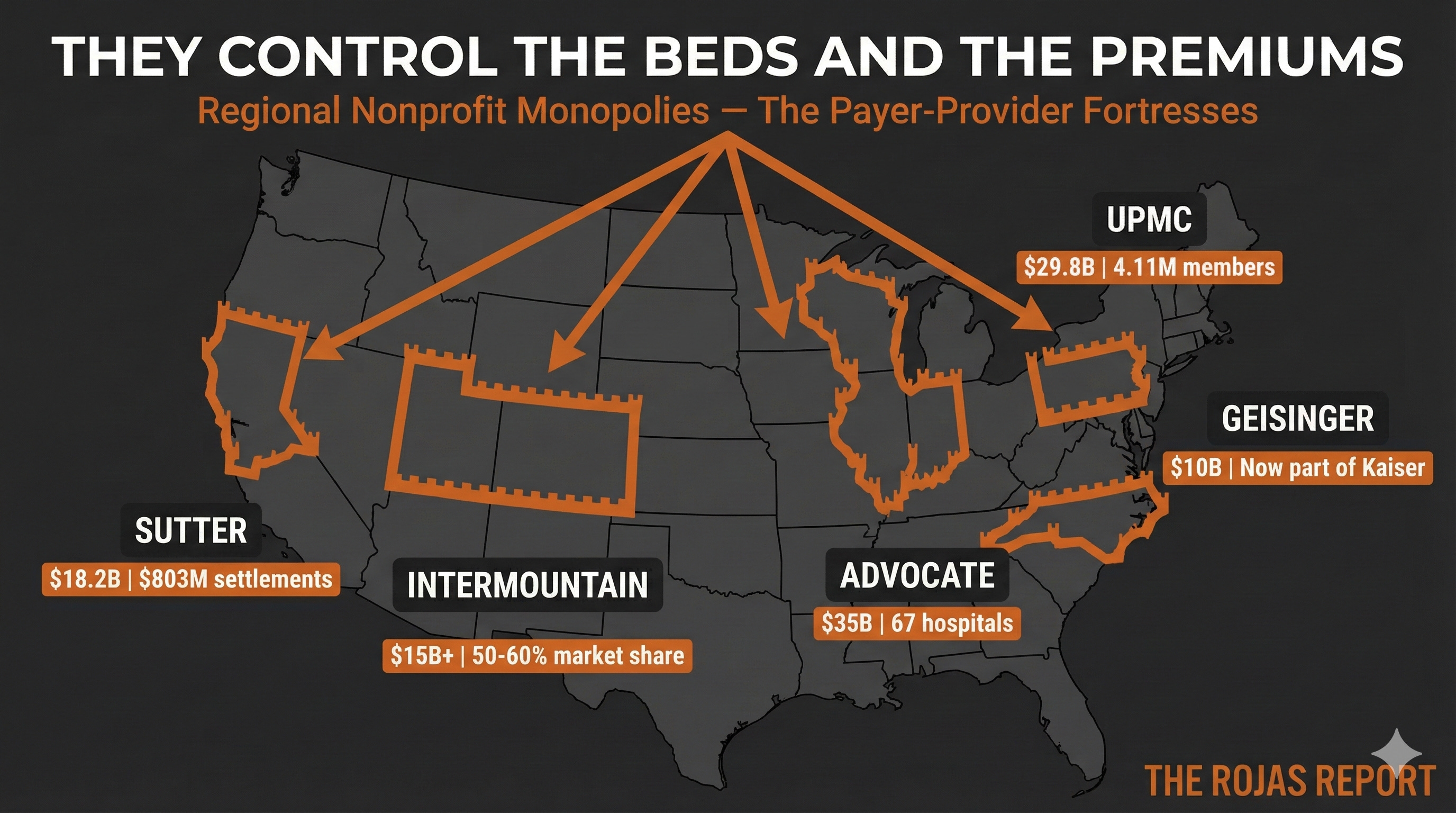
Regional Nonprofit Monopolies: The Payer-Provider Fortresses
They Asked Kaiser’s Question. Then They Went to War. (Dynasty Day 4)

$803 million.
That’s roughly equivalent to the annual salary of 12,000 teachers, or it could fund approximately 16,000 life-saving cancer treatments.
That’s how much one nonprofit hospital system has paid in antitrust settlements.
Not a for-profit. Not private equity. A tax-exempt “charitable” organization.
They didn’t pay because they got caught being inefficient.
They paid because they got caught fixing prices.
And they’re not alone.
This is Part 4 of the Five Dynasties series.
We’ve covered Kaiser (the integration template), the Academic Medical Centers (the prestige cartel), and the Catholic Systems (the cross-market consolidators).
Today: the regional nonprofits that took Kaiser’s model and weaponized it.
The Question Nobody Would Say Out Loud
In the 1990s, the executives at the University of Pittsburgh Medical Center asked a question that changed American healthcare:
If we’re the dominant hospital system, why are we letting an insurance company skim the premium?
So they built their own health plan.
Then they went to war.
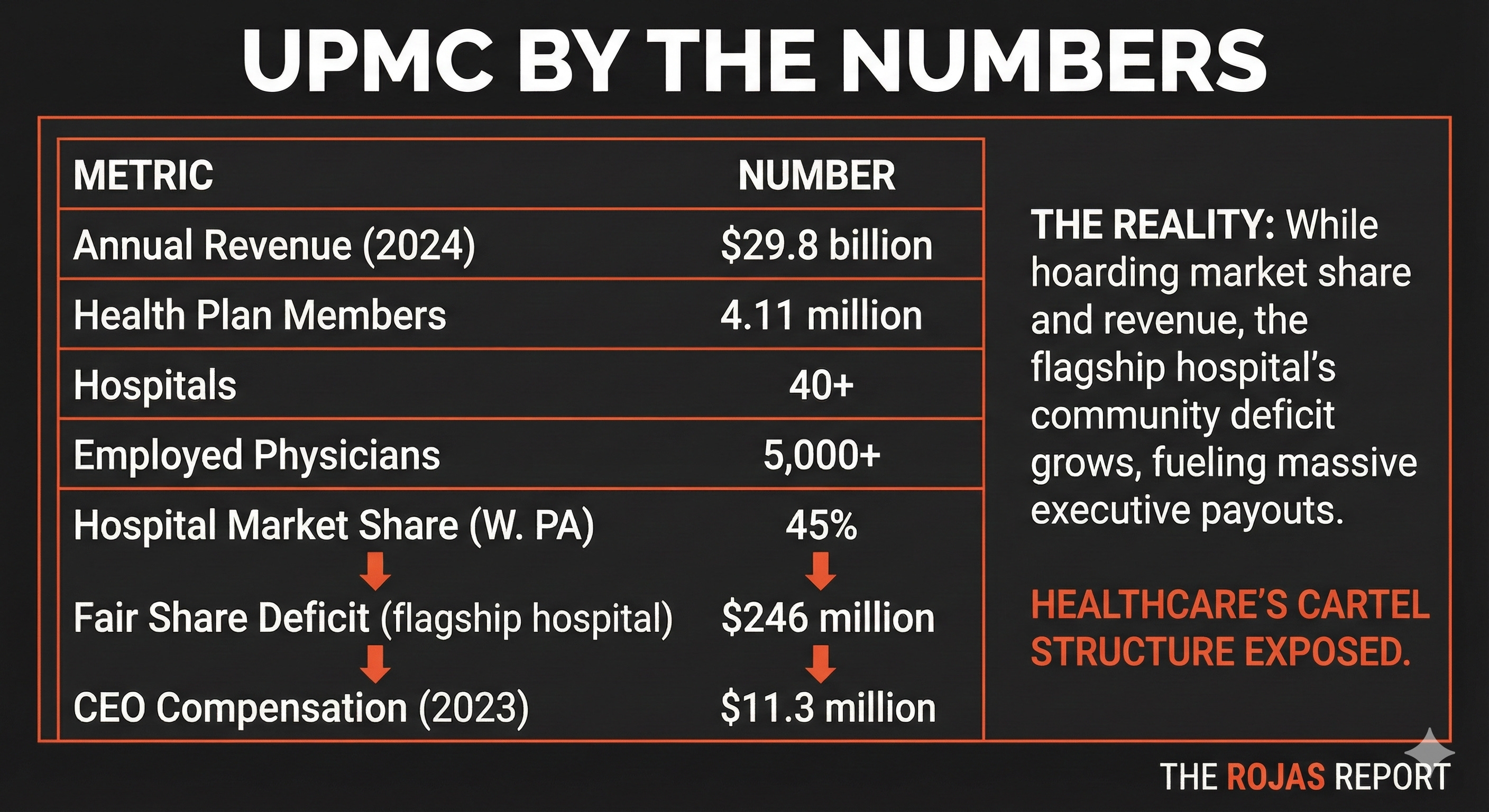
UPMC: The Archetype
UPMC didn’t just compete with Highmark, the region’s dominant Blue Cross insurer.
They declared war.
The timeline:
UPMC announced it would stop accepting Highmark patients. Hundreds of thousands of people, including cancer patients, seniors on Medicare Advantage, and families with chronic conditions, faced losing access to their doctors.
A study found that during this period, there was a 25% increase in emergency room visits among these patients due to the disruption of their regular care.
Additionally, there was a reported 15% increase in hospital readmissions within the first three months of the policy change.
The state intervened. Lawsuits. Consent decrees.
Years of chaos for patients caught in the crossfire.
UPMC won.
The Hostage Tactic
When UPMC’s market dominance was challenged, patients became leverage.
Barbara Marsic, a breast cancer and MS patient in Pittsburgh, was told she’d have to choose between her insurance and the UPMC neurologist she’d seen for 15 years:
“I just hate the idea of losing the doctors I’ve seen for years. But it may cost too much to stay with them.”
Evalyn Bodick, a 74-year-old breast cancer survivor, was told she’d have to pay cash to continue seeing the UPMC doctors who saved her life:
“I don’t have the money to do that. It’s a kind of extortion.”
This isn’t a for-profit insurance company using patients as pawns.
This is a nonprofit hospital system.
The Truce That Wasn’t a Victory
In 2019, Pennsylvania’s Attorney General sued UPMC for “anticompetitive behavior,” invoking its charitable obligations as a nonprofit.
Under pressure, UPMC and Highmark signed a 10-year truce that restored in-network access.
But UPMC emerged with its dominance intact. It controls the beds. It controls the premiums. Employers in Western Pennsylvania have no choice, if they want employees to access UPMC hospitals, they have to offer the UPMC plan.
And UPMC Health Plan denies claims.
It has prior auths. It uses utilization management.
It’s just called a “nonprofit integrated delivery system” instead of a “health insurer.”
The scrutiny is different.
The behavior is the same.
The Playbook Spreads
UPMC proved the model. Others followed.
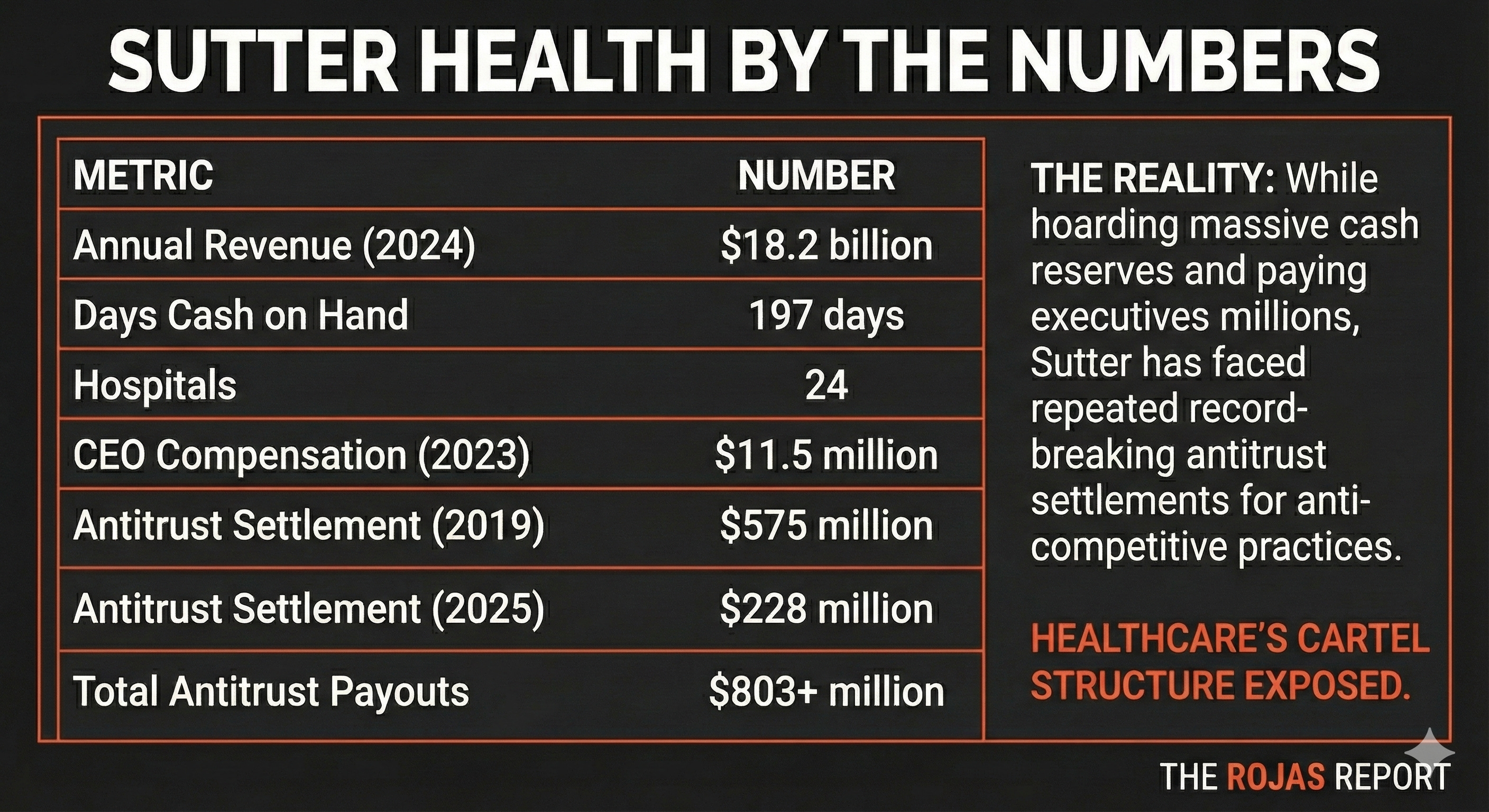
Sutter Health: The Price-Fixer
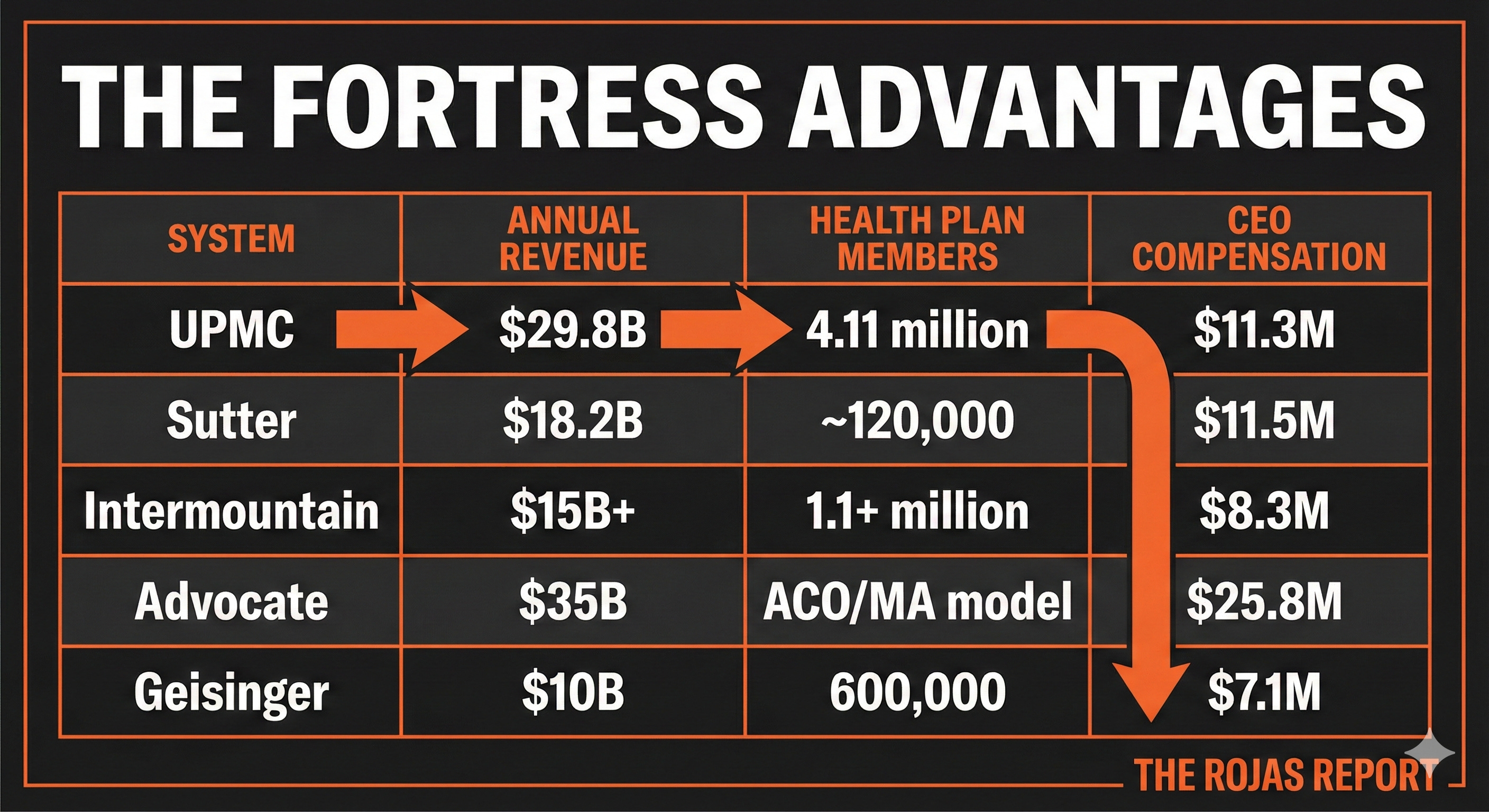
$803 million.
That’s how much Sutter Health has paid in antitrust settlements.
In Northern California, Sutter built a monopoly through tactics so egregious that the state sued:
All-or-nothing contracting: Insurers had to include ALL Sutter facilities or NONE — even the overpriced ones.
Gag clauses: Contracts prohibited insurers from telling patients that Sutter was more expensive than alternatives.
Anti-steering rules: Insurers couldn’t direct patients to lower-cost competitors.
The result?
Having a baby in Sutter’s territory costs nearly twice as much as in Los Angeles. In addition to the increased patient costs, employers also face significant financial challenges.
For example, regional employers have reported a 15% hike in insurance premiums, passing some of the burden of Sutter’s market dominance onto their businesses. This creates a ripple effect, impacting hiring capabilities and overall economic growth in Northern California.
Sutter-affiliated OB-GYNs were reimbursed 3x more than independent physicians for the same service.
Northern California prices run 20-30% higher than Southern California, a direct result of Sutter’s market dominance.
As one employer coalition leader testified during the trial:
“Sutter made themselves the only game in town, and they made us pay for it.”
California’s AG put it plainly: “We seek to stop Sutter from continuing this illegal conduct.”
Sutter settled. It agreed to end the all-or-nothing contracting.
It accepted 10 years of compliance monitoring.
But its network remains intact.
Its market power endures.
The fine was the cost of doing business.
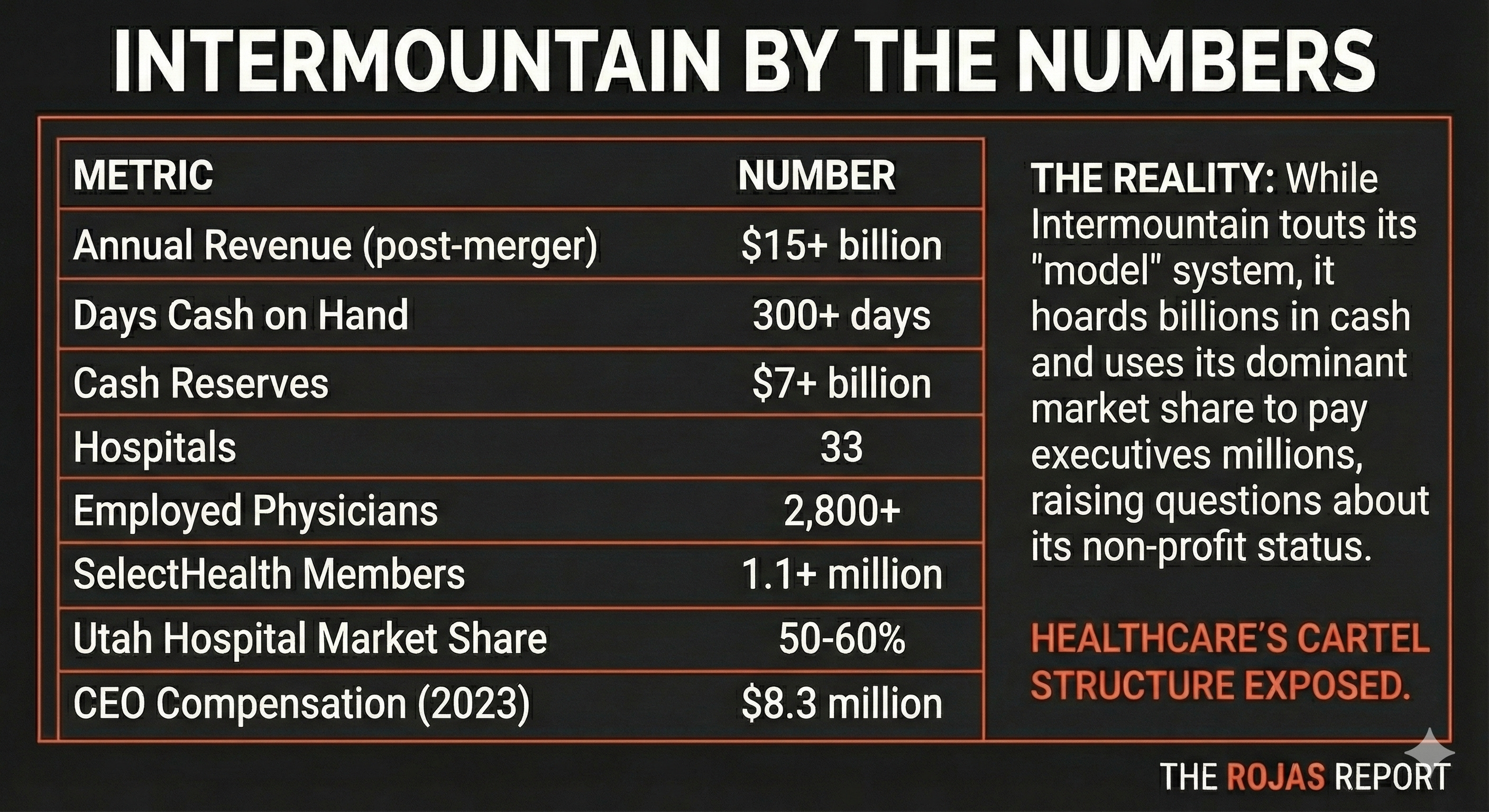
Intermountain Health: The Quiet Expansionist
Intermountain doesn’t make headlines like UPMC or Sutter.
That’s by design.
From its stronghold in Utah, a state without CON laws, Intermountain built the most profitable integrated system in the Mountain West. Then it started expanding.
Intermountain’s playbook is quieter but no less effective:
2022: Merged with SCL Health, adding Colorado and Montana to its empire.
2020: Proposed a 70-hospital merger with Sanford Health (it fell apart, but the ambition was clear).
SelectHealth, Intermountain’s insurance arm, accounts for roughly half of the system’s revenue.
It’s not a side business.
It’s the engine.
Even the DOJ took notice. In 2020, regulators blocked Intermountain’s attempt to acquire a minority stake in a competing community hospital, arguing that even a minority stake would “reduce incentives to compete.”
Intermountain settled by slashing its stake to 7.5%.
But the message was clear: even in a state without CON laws, market power is the ultimate barrier to entry.
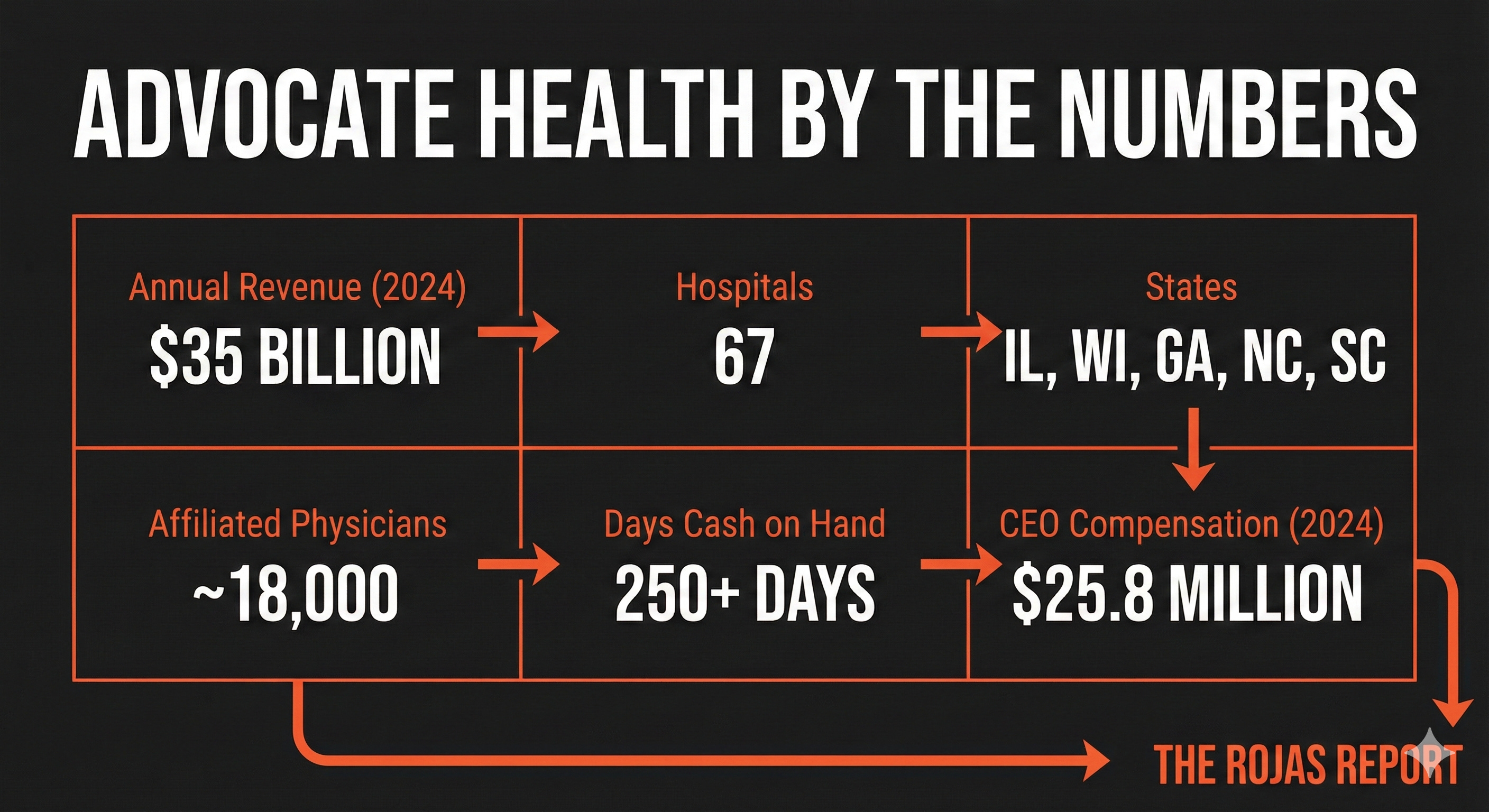
Advocate Health: The Stealth Monopoly
In December 2022, Advocate Aurora (the largest system in Illinois and Wisconsin) merged with Atrium Health (the dominant system in North Carolina).
The result: $35 billion in revenue. 67 hospitals. 18,000 physicians.
The FTC didn’t challenge it.
Why?
No geographic overlap.
This is the new playbook: cross-market mergers.
Research shows that when hospital systems acquire facilities in different markets within the same state, prices still jump 7-10%. The theory is simple: insurers that serve employers across multiple regions now face a single negotiating counterparty with leverage in all of them.
As one 2019 study warned:
“Since insurers serve employers across multiple regions, a merged cross-market hospital system that covers those regions can demand higher reimbursement rates.”
Atrium (now part of Advocate) already had a history of anticompetitive behavior. In 2018, the DOJ and North Carolina AG forced Atrium to stop using anti-steering clauses — contract provisions that prevented insurers from directing patients to lower-cost competitors.
The DOJ noted that Atrium was the “dominant hospital system in the Charlotte area” and that its tactics had resulted in higher costs for consumers.
Now that dominant system is part of a multi-state colossus.
The fortress walls just got higher.
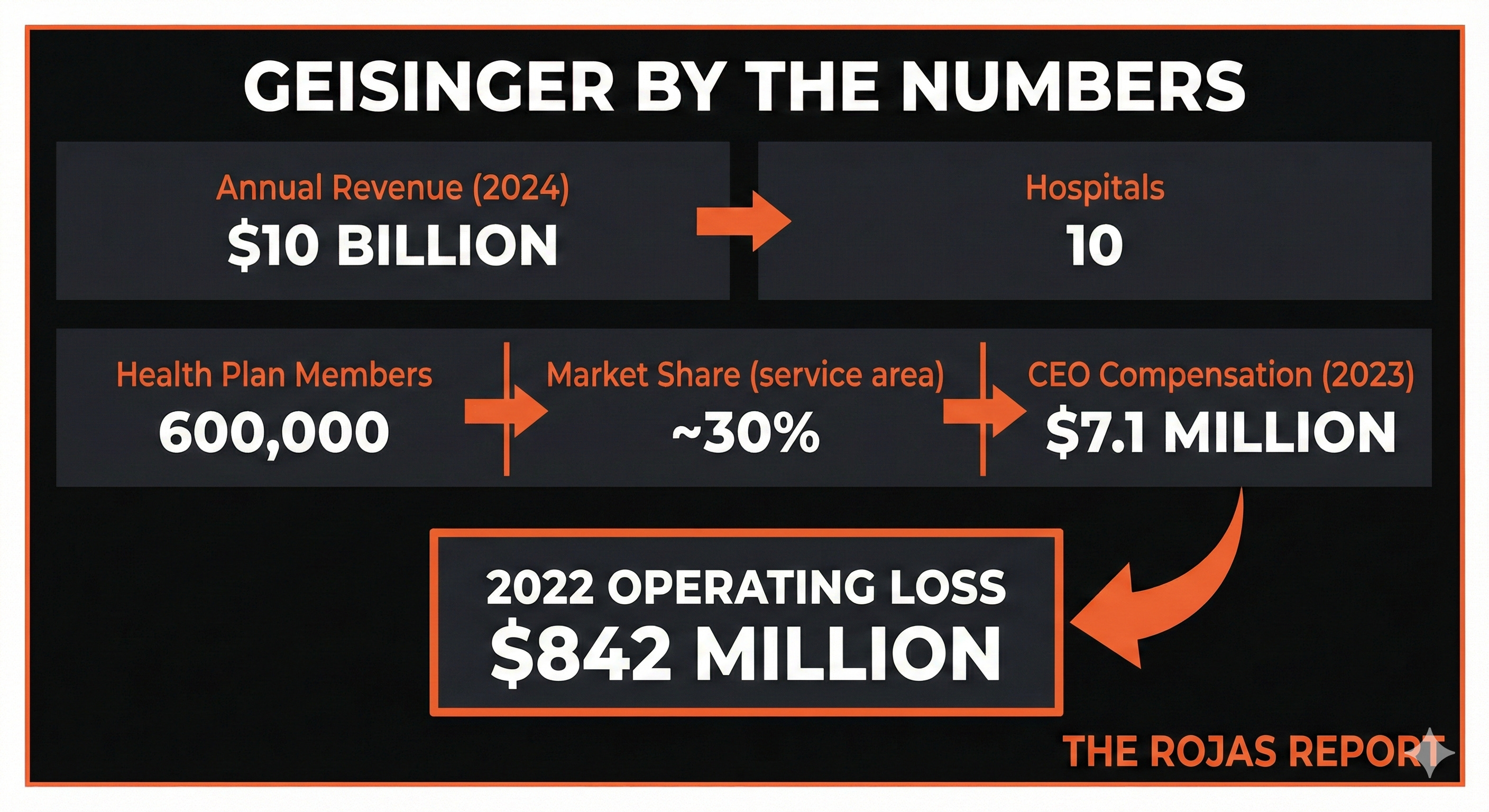
Geisinger: The First Domino
Geisinger was supposed to be different.
The Pennsylvania system was a pioneer of value-based care, the ProvenCare bundled payment model, advanced EHR adoption, and even a “Fresh Food Farmacy” addressing food insecurity.
But Geisinger was also struggling. An $842 million loss in 2022. Encroachment from UPMC and Penn State Health. A health plan that was innovative but small.
So Geisinger did something unprecedented: it surrendered its independence.
In 2023, Geisinger agreed to join Risant Health, a new subsidiary of Kaiser Permanente.
The deal closed in 2024. Kaiser recorded a $4.6 billion accounting gain.
But here’s what matters:
Risant Health plans to acquire 5-10 more regional systems.
Kaiser, the original integrated nonprofit, is now exporting its model nationwide. Geisinger is the first domino in a plan to create a national network of regional fortresses under a single strategic umbrella.
The Kaiser model isn’t just being imitated anymore.
It’s being franchised.
The Evidence Is Clear
A 2024 literature review on vertical integration in healthcare concluded:
“Vertical integration has yielded inconsistent effects on quality… but has consistently driven up prices.”
The promise was coordinated care. Lower costs. Better outcomes.
The reality is market power. Margin capture. Monopoly.
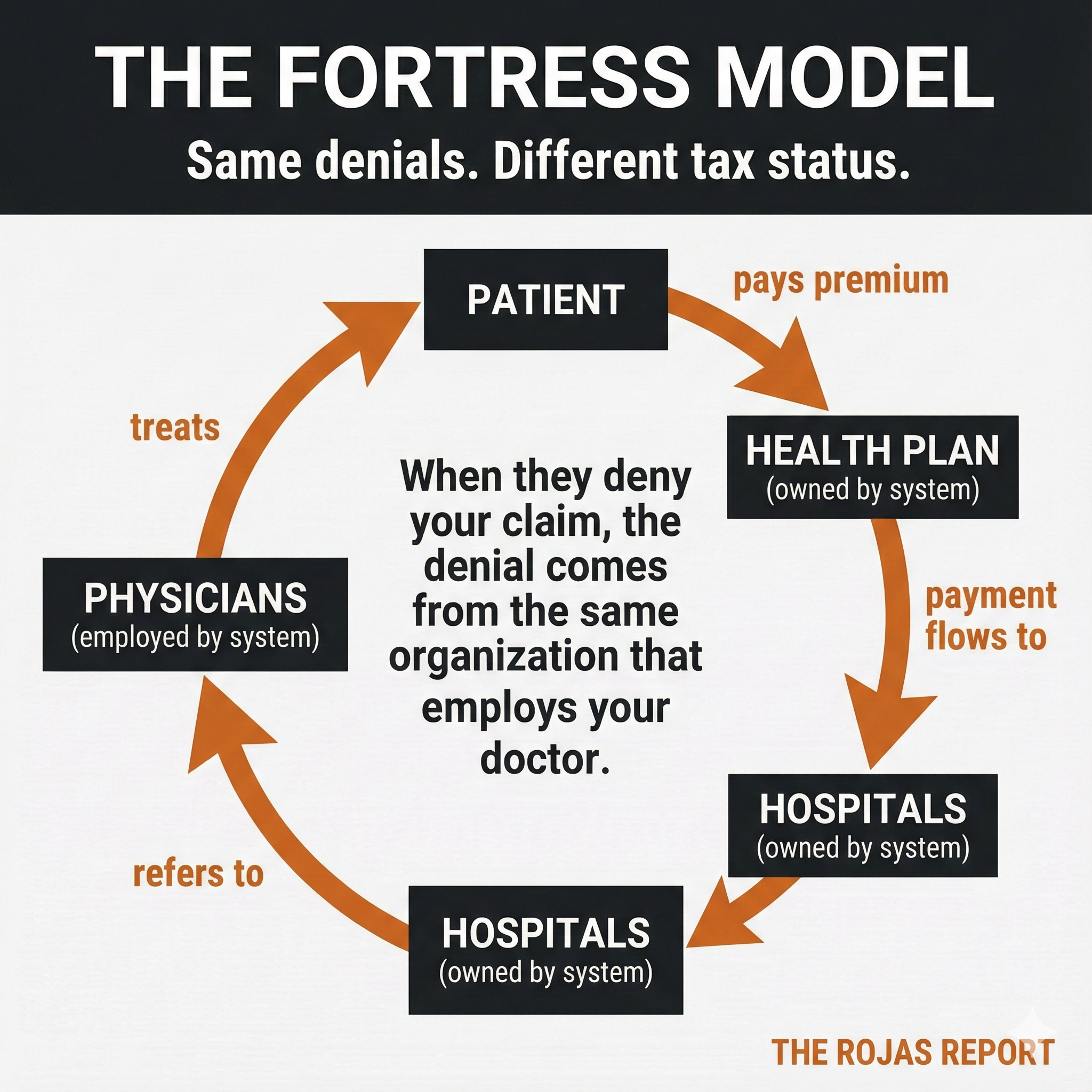
The Conflict of Interest Nobody Talks About
When UPMC Health Plan denies your MRI, that’s not Aetna.
That’s the health system.
When Sutter’s insurance arm refuses a referral to a competitor, the savings don’t go to some faceless corporation. They stay inside Sutter. When Intermountain’s SelectHealth says your drug isn’t covered, the system that employs your doctor is the same system that made that decision.
As an open question, consider whether denial rates differ measurably between integrated systems like these and stand-alone insurers. It’s worth investigating whether patients in integrated systems experience higher denial rates and whether these systems provide better or worse outcomes. Such questions call for data-driven analysis, inviting readers to explore this potential conflict of interest more deeply.
One Geisinger patient put it simply:
“At Geisinger, the doctor and insurer might share a logo, but that didn’t get my MRI approved any faster.”
The psychological promise of integration is seamless care.
The financial reality is seamless control.
What the Regulators Said
DOJ Antitrust (2019): “We are seeing the Kaiser model imitated in ways that reduce competition without delivering Kaiser’s benefits.”
Pennsylvania AG: “Nonprofit status is not a license to hurt patients.”
FTC Commissioner (2022): Payer-provider combinations can create “fortresses against entry” — new insurers can’t break in because the dominant provider won’t contract with them, and new providers can’t get patients because the dominant insurer steers members internally.
The Pattern
Every regional monopoly followed the same playbook:
Step 1: Consolidate the hospitals.
Step 2: Build or buy a health plan.
Step 3: Make yourself unavoidable — employers must include you or face employee revolt.
Step 4: Use the insurance arm to keep referrals internal and capture the margin that used to go to external insurers.
Step 5: When challenged, use patients as leverage. Make the alternative (losing access) unthinkable.
Step 6: Settle if you must. Pay the fine. Keep the fortress.
This is the Kaiser model, weaponized.
The Bottom Line
These regional nonprofits asked Kaiser’s question: If we control the beds, why let the insurers take the margin?
So they built their own health plans.
They went to war with incumbent insurers.
They won.
Now they control both the delivery and the denial.
When the UPMC Health Plan says no to your scan,
that’s not some insurance company in another state.
That’s the hospital.
Same denials.
Same prior auths.
Same moats.
Different tax status.
Tomorrow: Dynasty 5
The 340B Empires, The Safety-Net Exploiters.
A program designed to help hospitals serving the poor became a $54 billion spread trade.
One oncologist can generate $1 million in annual 340B profit for a hospital.
Child sites exploded from 1,339 to 36,000+.
The patients they serve?
Increasingly wealthy.
The moats stack.
The entire non-profit industry needs to be dismantled. Many non-profits start out with good intentions, but it doesn’t take long for them to morph into little — and big — monsters. We’ve seen this at every level from humane societies and bunny rescues to massive hospital and insurance systems you describe. Of course, the chance of repealing 501(c)(3) laws is nil; but 501(c)(3) organizations that are abusing the original intention of this tax code must lose their non-profit status — IMMEDIATELY if not sooner.
We have repeatedly urged legislators to oppose bills that donated taxpayer dollars to selected charities. We have consistently opposed government giving taxpayer money to non-profits and non-government organizations.
This is taxation without representation. This is selective public charity forced on taxpayers. And, because many non-profits such as so-called “charitable” (but very rich) hospitals pay little or no property taxes, other property owners must take up the slack for ever hungrier government activities.
We wish the entire non-profit industry would lose non-profit status and let individuals decide whether to support them financially — not because donors get tax breaks, but because they truly believe in the mission and the people behind the organization they're funding.
Taxpayer money should not be funding “charitable” or non-government organizations (NGOs). And charitable organizations should lose all special tax breaks, as they've generally abused privileges the tax code granted.
Americans have seen too much corruption — e.g., USAID, hospital systems, universities, bio-pharmaceutical industrial complex, military-industrial complex, and more — to continue supporting the non-profit and non-government organization cartels.