
Single-Payer Is Surrender. The Status Quo Is No Victory Either.
Why the healthcare debate is trapped in a false binary, and what replaces it.

A healthcare system designed to suppress competition is not failing.
It’s working exactly as intended.
The American healthcare debate is trapped in a false binary.
On one side sits single-payer: the promise that centralized government administration will finally rationalize costs, expand access, and restore fairness.
On the other side sits the status quo, defended (often reflexively) as the product of “free markets,” competition, and private enterprise.
Neither description is accurate.
And neither option addresses the structural causes of failure.
The result is an argument that goes in circles while costs rise, competition disappears, and institutional power consolidates.
In today’s article:
Why single-payer creates a government monopsony that eliminates physician exit options
How Congressman Ro Khanna’s August 2025 legislation reveals what “Medicare for All” actually means for independent practice
The low-hanging fruit Republicans refuse to pick: physician-owned hospitals, site-of-service arbitrage, and CMS price-setting
What replaces both failed options: parallel structures that render the cartel obsolete
Glossary of terms at the bottom.

A System That Defies Comparison
Illegal drug cartels generate an estimated $40 billion annually.
American healthcare absorbs roughly $5.7 trillion.
The comparison is not moral; it is structural. Both suppress competition. Both capture regulators. One operates outside the law and is prosecuted accordingly. The other operates within a dense legal framework that confers protection, tax exemption, and regulatory authority on its largest participants.
Understanding that distinction matters. Because healthcare’s dysfunction is not the result of neglect or mismanagement. It is the predictable outcome of a system designed to suppress competition while preserving the appearance of pluralism.
This is not an accusation of malice. It is a recognition of incentives.
The Limits of the Single-Payer Argument
Single-payer proposals are typically framed as moral correctives: universal coverage, administrative simplicity, equity through uniformity.
But single-payer systems are, by definition, systems of centralized authority. One payer implies one rule-maker, one reimbursement schedule, one arbiter of medical necessity.
History offers ample reason for caution when such authority is consolidated.
The federal government has repeatedly demonstrated that it is capable of prolonged institutional error (sometimes catastrophic) without meaningful accountability. From public health failures to foreign policy misadventures to financial crises, administrative confidence has often exceeded institutional competence.
In healthcare, this matters profoundly. Decisions about coverage, prioritization, and access do not require overt coercion to shape behavior. Administrative discretion alone is sufficient.
Coverage can be delayed.
Eligibility criteria can be narrowed.
Reimbursement rules can condition behavior.
Advocates often assume benevolence will be permanent. History suggests otherwise.
The irony is striking: Americans routinely express fear about executive overreach, yet are encouraged to place complete authority over healthcare into the hands of whichever administration happens to prevail next.
That is not reform. It is concentration risk. And in a sector as vital and complex as healthcare, that risk is not theoretical.
The Quiet Part Out Loud: What Single-Payer Means for Physician Independence
California Congressman Ro Khanna has been one of the most vocal advocates for Medicare for All. In August 2025, he and Senator Ed Markey reintroduced the State-Based Universal Health Care Act. The bill would allow states to bundle Medicare, Medicaid, ACA, Tricare, and VA dollars into state-level single-payer systems.
Khanna frames this as “state innovation.” The framing obscures what it actually is: a path to government monopsony over medicine.
Single-payer advocates will tell you that physicians can still operate “private practices” under their system. Technically true. Economically meaningless.
Under single-payer, there is one payer. One rate-setter. One arbiter of what constitutes “medically necessary.”
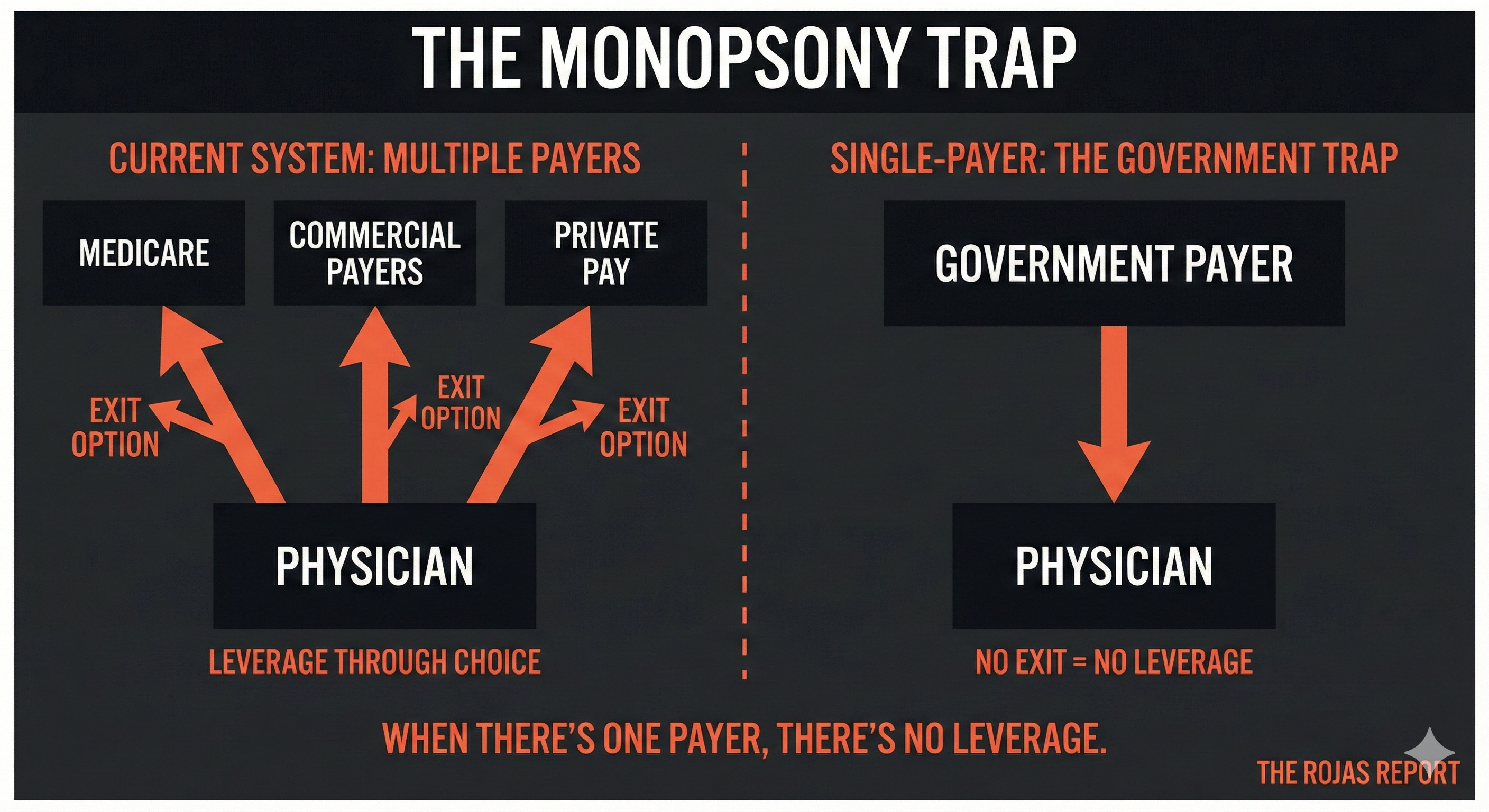
Today, a physician who finds Medicare rates unsustainable can decline Medicare patients and build a practice around private-pay or commercial insurance. That exit option disciplines the system. It creates a floor below which government payment cannot fall without losing physician participation.
Single-payer eliminates that exit.
When there are no private-pay patients, there is no leverage. When there is no leverage, “private practice” becomes a semantic distinction without practical meaning. You are an independent contractor with one client who sets all terms.
The Heritage Foundation put it bluntly: under single-payer, “The only alternative for a physician would be to cease the practice of medicine.”
Khanna appeared on CNBC in October 2025, arguing that Medicare doesn’t ration care as private insurers do. He pointed to pre-authorization burdens from commercial payers as evidence that government administration is more physician-friendly.
He’s half right. Private insurers do impose burdensome pre-authorization. They do deny claims. They do interfere with clinical judgment.
But Khanna’s argument assumes the solution to one form of administrative interference is total dependence on another. It trades the dysfunction of fragmented payer bureaucracy for the dysfunction of monopolized payer bureaucracy.
The question is not whether private insurance is good. It isn’t.
The question is whether concentrating all payment authority in a single government entity creates better conditions for physician autonomy, or worse ones.
History and institutional behavior suggest worse.
The status quo has a tremendous advantage: it doesn’t need to be explained. It simply exists. It’s the default. Defaults win almost every time because choosing something else requires effort, and effort requires a reason.
This article is the reason.
You now have two choices. Return to the default and forget what you read by Thursday. Or subscribe and become the sort of person who makes other people uncomfortable at conferences.
60,000+ physicians chose discomfort. The Rojas Report. It’s not for everyone. That’s rather the point.
The Myth of Free Markets in American Healthcare
If the left overestimates the virtues of centralization, the right routinely misrepresents the nature of the existing system.
Healthcare in the United States does not function as a free market in any meaningful economic sense. Prices are opaque. Entry is restricted. Exit is regulated. Competition is routinely blocked.
This is not accidental.
A question for Republicans who invoke free markets as their defense of the status quo: Do you understand what a market actually is?
Markets require prices. Not charges. Not negotiated rates buried in contracts. Prices. Visible, comparable, meaningful signals that allow buyers and sellers to make informed decisions.
Prices are how markets communicate. They signal scarcity. They signal value. They create benchmarks against which alternatives can be measured.
Healthcare has none of this.
Do Republicans understand what commodities exchanges do? Why does the Chicago Mercantile Exchange exist? Why can farmers hedge corn futures, and airlines can hedge jet fuel?
Because someone built the infrastructure for price discovery, someone created the marketplace where buyers and sellers could transact transparently.
Amazon did this for retail. Kayak did it for airfare. Expedia did it for hotels. CarGurus did it for used cars.
Where is the equivalent for healthcare?
It doesn’t exist. And the policies Republicans have written, the regulations they’ve preserved, and the lobbyist donations they’ve accepted ensure it never will.
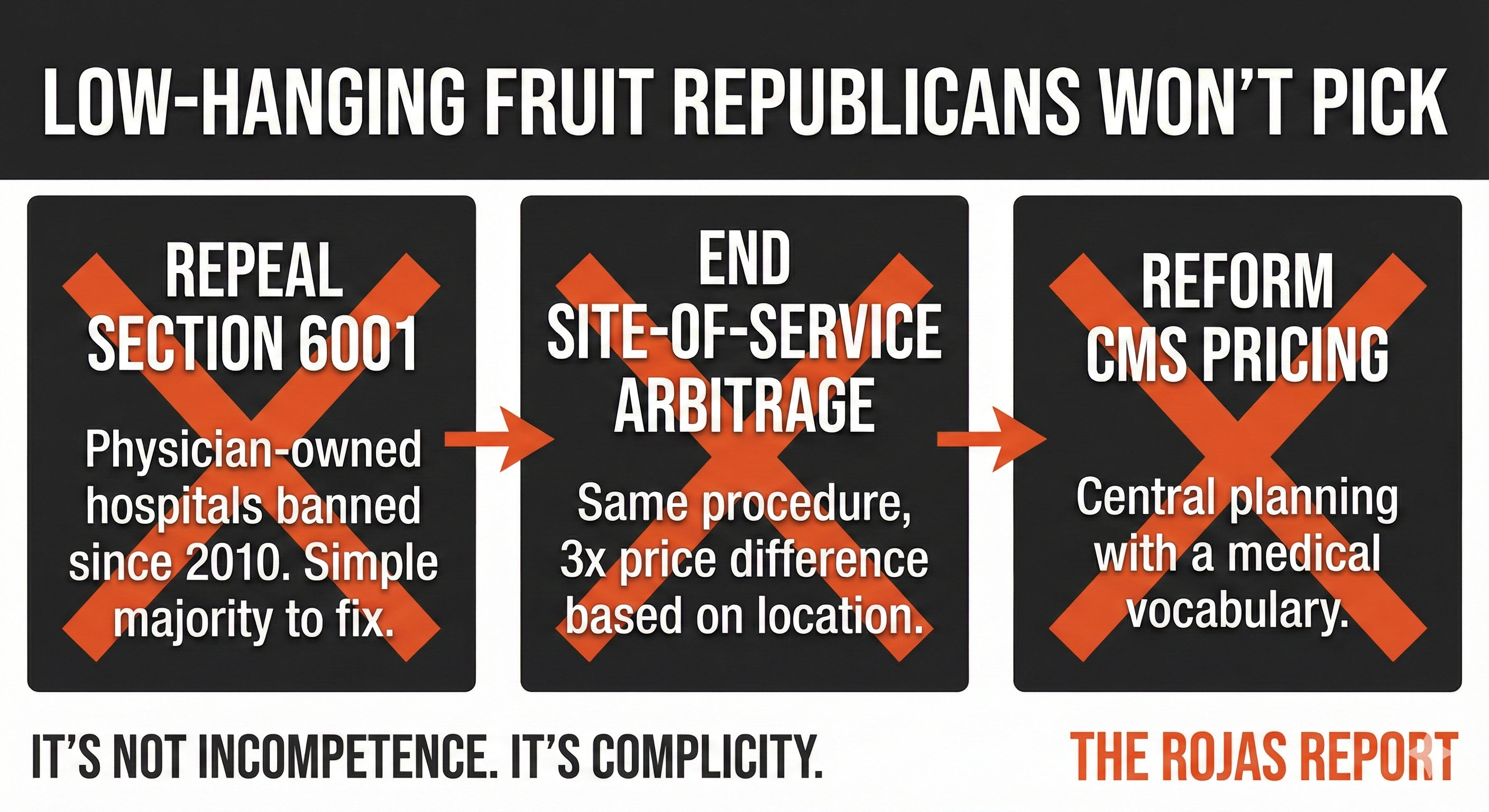
Consider the low-hanging fruit:
The physician-owned hospital moratorium. Section 6001 of the Affordable Care Act banned new physician-owned hospitals and froze existing ones in 2010. The data showed these facilities delivered better outcomes at lower costs. Congress banned them anyway.
Republicans have controlled the House, the Senate, and the White House multiple times since 2010. Repealing Section 6001 requires a simple majority. It would increase supply. It would introduce competition. It would lower prices.
Basic economics. Supply and demand. More supply, lower prices.
They haven’t done it.
Site-of-service arbitrage. CMS pays dramatically different rates for identical procedures based on where they’re performed. A colonoscopy at a hospital outpatient department can cost three times what it costs at an ambulatory surgery center. Same physician. Same equipment. Same patient. Different price.
This is not a market outcome. This is an administrative decision. CMS created this distortion. CMS could eliminate it.
Republican administrations have had ample opportunity to direct CMS to equalize site-of-service payments. They haven’t done it.
Central planning at CMS. The agency sets prices for thousands of procedures using the Resource-Based Relative Value Scale. Committees meet. Formulas are applied. Prices are announced.
This is not price discovery. This is central planning with a medical vocabulary.
A market-oriented approach would use actual transaction data. It would create exchanges where prices emerge from supply and demand. It would employ mean reversion models based on real-world outcomes, not committee estimates.
The infrastructure exists. We use it for commodities. We use it for equities. We use it for airline tickets.
CMS could transition from price-setter to market facilitator. Republican administrations have never attempted it.
Over the past half-century, Republican administrations have controlled Congress and the presidency in nearly every possible configuration. Yet the structural impediments to competition remain firmly in place.
Certificate of Need laws (widely recognized as protectionist since the 1980s) still restrict entry in most states.
Price transparency rules exist largely without enforcement.
Vertical consolidation continues unabated.
Intermediaries extract rents with minimal oversight.
You cannot claim to support free markets while preserving every barrier that prevents them from functioning.
The explanation is not ideological failure. It is political economy: the predictable result of institutional incentives shaped by entrenched interests.
The System Is Not Broken. It Is Working as Designed.
Healthcare’s defenders often speak of “misaligned incentives” or “unintended consequences.” This understates the problem.
The system functions precisely as its rules encourage.
Hospitals can veto competitors.
Employment models are favored over independent practice.
Price competition is discouraged while consolidation is rewarded.
Regulatory exemptions protect incumbents while criminal liability deters challengers.
This is not a failure of capitalism. It is the suspension of it.
When outcomes are examined through this lens, the persistence of high prices, restricted access, and declining physician autonomy becomes entirely predictable.
The Real Alternative Is Structural, Not Political
History suggests that entrenched systems rarely reform themselves through legislation alone. They are more often displaced by parallel structures that operate outside the constraints incumbents impose.
Healthcare is no exception.
Price transparency that is voluntary, searchable, and meaningful; not symbolic compliance.
Direct care models that eliminate unnecessary intermediaries.
Physician ownership structures that align incentives with outcomes.
Market infrastructure that allows real price discovery in medical services, as exists in nearly every other sector of the economy.
These approaches do not require permission. They require construction.
The prohibition on physician-owned hospitals in 2010 was not imposed because they failed. It was imposed because they succeeded, producing lower costs and better outcomes in ways the incumbent system could not control.
That historical detail matters.
Conclusion: Refusing the False Choice
Single-payer represents surrender to centralized authority.
The status quo represents surrender to cartelized power.
Neither deserves default allegiance.
Competition, not control, has historically disciplined costs and improved quality.
Pluralism, not monopoly, has preserved resilience in complex systems.
Construction, not rhetoric, has produced durable reform.
Healthcare will not be transformed by choosing between two flawed poles of the same debate. It will change when parallel systems make the existing structure impossible to defend.
Cartels do not collapse at the ballot box.
They collapse when alternatives render them obsolete.
That process has already begun.
Here’s an under appreciated fact: people don’t change their minds because of new information. They change their minds because someone they respect changed theirs first.
This is why forwarding matters more than reading. Your colleagues trust you. They don’t trust a newsletter they’ve never heard of. But they’ll trust a newsletter you sent them at 6am with the note “this explains everything.”
Be that person.
60,000+ physicians read The Rojas Report. Most of them became the person who explains things. Subscribe. Then forward. That’s the entire strategy.
- Rojas out

.
Glossary of Terms
Single-payer: A healthcare financing system in which a single entity (typically government) pays for all medical services. Physicians may remain in private practice, but all payment flows through one source.
Monopsony: A market structure with only one buyer. In healthcare, single-payer creates a monopsony where the government is the sole purchaser of medical services, eliminating physician leverage over payment rates.
State-Based Universal Health Care Act: Legislation introduced by Rep. Ro Khanna (D-CA) and Sen. Ed Markey (D-MA) allowing states to bundle federal healthcare dollars (Medicare, Medicaid, ACA, Tricare, VA) into state-level single-payer systems.
Section 6001: Provision of the Affordable Care Act (2010) that banned new physician-owned hospitals and froze the expansion of existing ones. Justified as preventing self-referral, functionally eliminated a competitive threat to hospital systems.
Site-of-service arbitrage: The practice of CMS paying different rates for identical procedures based on where they are performed (e.g., hospital outpatient department vs. ambulatory surgery center), creating price distortions unrelated to quality or cost.
Resource-Based Relative Value Scale (RBRVS): The formula CMS uses to set Medicare physician payment rates. Prices are determined by the committee’s estimate of resources required, not by market transaction data.
Certificate of Need (CON) laws: State regulations requiring healthcare providers to obtain government approval before building new facilities or expanding services. Incumbent competitors typically have standing to challenge applications.
Price discovery: The market process by which prices are determined through the interaction of buyers and sellers. Absent in healthcare due to opaque pricing, third-party payment, and regulatory barriers.
Sources
Robert A. Book, “Single Payer: Why Government-Run Health Care Will Harm Both Patients and Doctors,” The Heritage Foundation, April 2009.
Rep. Ro Khanna and Sen. Ed Markey, “State-Based Universal Health Care Act,” reintroduced August 2025.
Rep. Ro Khanna, CNBC “Squawk Box” appearance, October 2025.
Section 6001, Patient Protection and Affordable Care Act, 42 U.S.C. § 1395nn (2010).
60,000+ physicians and healthcare operators read The Rojas Report daily. Join them.