
SUNDAY THOUGHT: ROME, AMERICA, AND THE HEALTHCARE CARTEL
1913: The Year They Rewired the Republic. The Healthcare Cartel Is What They Built With It.

February: the income tax.
April: popular election of senators.
December: a central bank drafted in secret by six men on a private island.
Every structural advantage the healthcare cartel holds today traces back to what was built on that foundation. The playbook is 1,800 years old. The American version took one year.
If you lived in Rome in 260 AD, your world was falling apart.
The currency in your pocket buys half as much as it did five years ago. The emperor had been captured by the Persians. The empire had fractured into three pieces. The legions were gone, replaced by mercenaries who fought for pay, not for Rome.
But the coins still carried the emperor’s face. The Senate still met. The propaganda said everything was fine.
If you’re a physician in America right now, this sounds familiar.
Your reimbursement buys less every year.
Your autonomy has been captured by hospital systems.
Independent medicine is fracturing state by state.
The gaps are filled by temporary labor and scope-expanded substitutes who bill at your rate for a fraction of the training you provide.
And the AMA still claims to represent you.
The coins still carry the emperor’s face.
This is the story of how that happened.
It starts in Rome.
It runs through 1913.
It ends in your waiting room.
IN TODAY’S ARTICLE:
How the Roman Empire fractured, debased its currency, diluted its titles, and outsourced its military to the people who would replace it. The same sequence is running in American healthcare right now.
1913: Jekyll Island, the 16th Amendment, the 17th Amendment, and the single calendar year that rewired the American republic into an operating system designed for capture.
The propaganda war that kept Roman citizens believing in an empire that had already stopped functioning, and the identical campaign the AMA, CMS, and hospital systems run today.
Why the healthcare cartel didn’t capture a functioning republic. It captured an administrative state that was already built for extraction. And what physicians can do about it.
Glossary at the bottom of today’s article.
IF YOU LIVED IN THE 3RD CENTURY, YOUR WORLD WAS FALLING APART
Imagine this.
You’re a Roman citizen in 260 AD. Your grandfather fought in the legions. Your father was a merchant who traded across three provinces under the protection of Roman law. You grew up believing the empire was permanent.
Now the currency in your pocket buys half what it did five years ago. The silver is gone. The coin is bronze with a wash. The emperor was captured by the Persians at Edessa. Captured. The most powerful man in the known world, dragged off in chains.
Postumus, a military commander in Gaul, declared himself emperor of the west. He took Gaul, Britannia, and Hispania. Zenobia, queen of Palmyra, took Syria, Egypt, and most of Asia Minor. The “real” emperor in Rome controlled Italy and not much else.
Three empires. One title. Nobody asked your permission.
The borders you grew up trusting are dissolving. Germanic tribes press from the north. Persians press from the east. The legions that once held the line have been replaced by foederati, barbarian mercenaries who fight for Rome because Rome can’t afford its own soldiers anymore.
The propaganda says everything is fine. The coins still carry the emperor’s face. The Senate still meets. The institutions still have names.
But you know. Everyone knows. The thing your grandfather believed in doesn’t exist anymore. What remains is the paperwork.
Now stop imagining. Because that’s Tuesday in American healthcare.
THE FRACTURE ALREADY HAPPENED
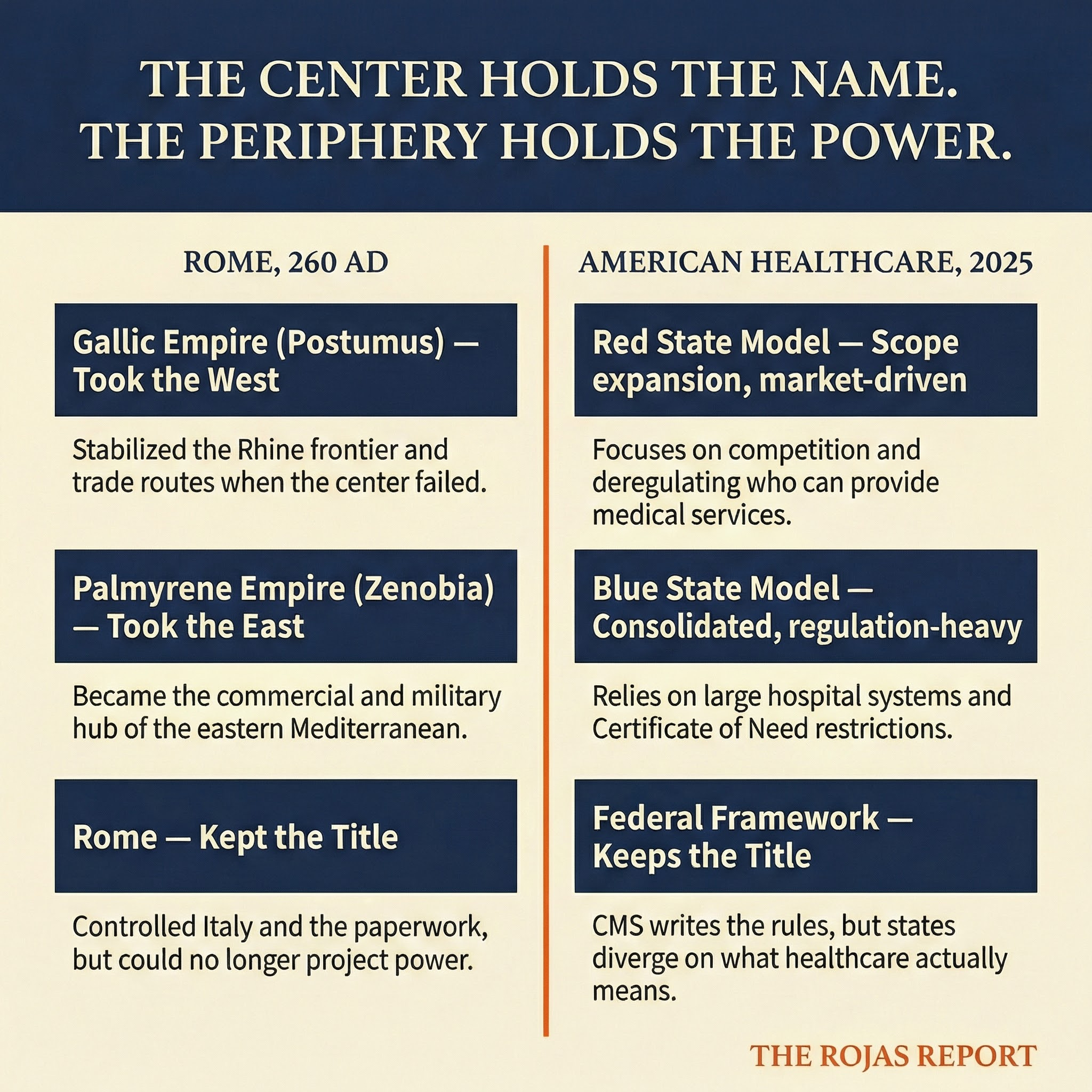
Postumus didn’t conquer the western provinces. He simply offered competence where Rome offered nothing.
The Gallic Empire wasn’t a rebellion. It was a service upgrade. Postumus stabilized the Rhine frontier, maintained trade routes, and minted better coins than Rome. The western provinces followed him because he delivered results. Rome didn’t.
Zenobia did the same thing in the east. Palmyra became the commercial and military hub of the eastern Mediterranean because the central government couldn’t project power past its own walls.
The fracture wasn’t violent overthrow. It was the periphery concluding that the center was no longer worth waiting for.
American healthcare fractured the same way. It just doesn’t have a name for it yet.
Texas has fundamentally different scope of practice laws, regulatory frameworks, and market structures than New York. California operates under different assumptions than Florida. Red states and blue states aren’t just diverging on politics. They’re diverging on what healthcare means, who delivers it, how it’s regulated, and who pays.
A physician practice in one state faces Certificate of Need laws, corporate practice of medicine restrictions, and scope limitations that don’t exist 50 miles across a state line. Same training. Same board certification. Different country.
The federal framework still exists on paper. CMS still writes the rules. But the lived reality is three or four competing healthcare systems wearing the same flag.
Postumus didn’t need to declare independence from Rome. He just needed to be more functional than Rome. The states doing their own thing in healthcare don’t need to secede. They just need to stop pretending Washington is steering.
They changed the word from “physician” to “provider” for the same reason Caracalla changed the word “citizen.” Not to include you. To extract from you. 60,000+ physicians see it now. Subscribe.
THE CARACALLA PLAY: HOW YOU KILL A TITLE
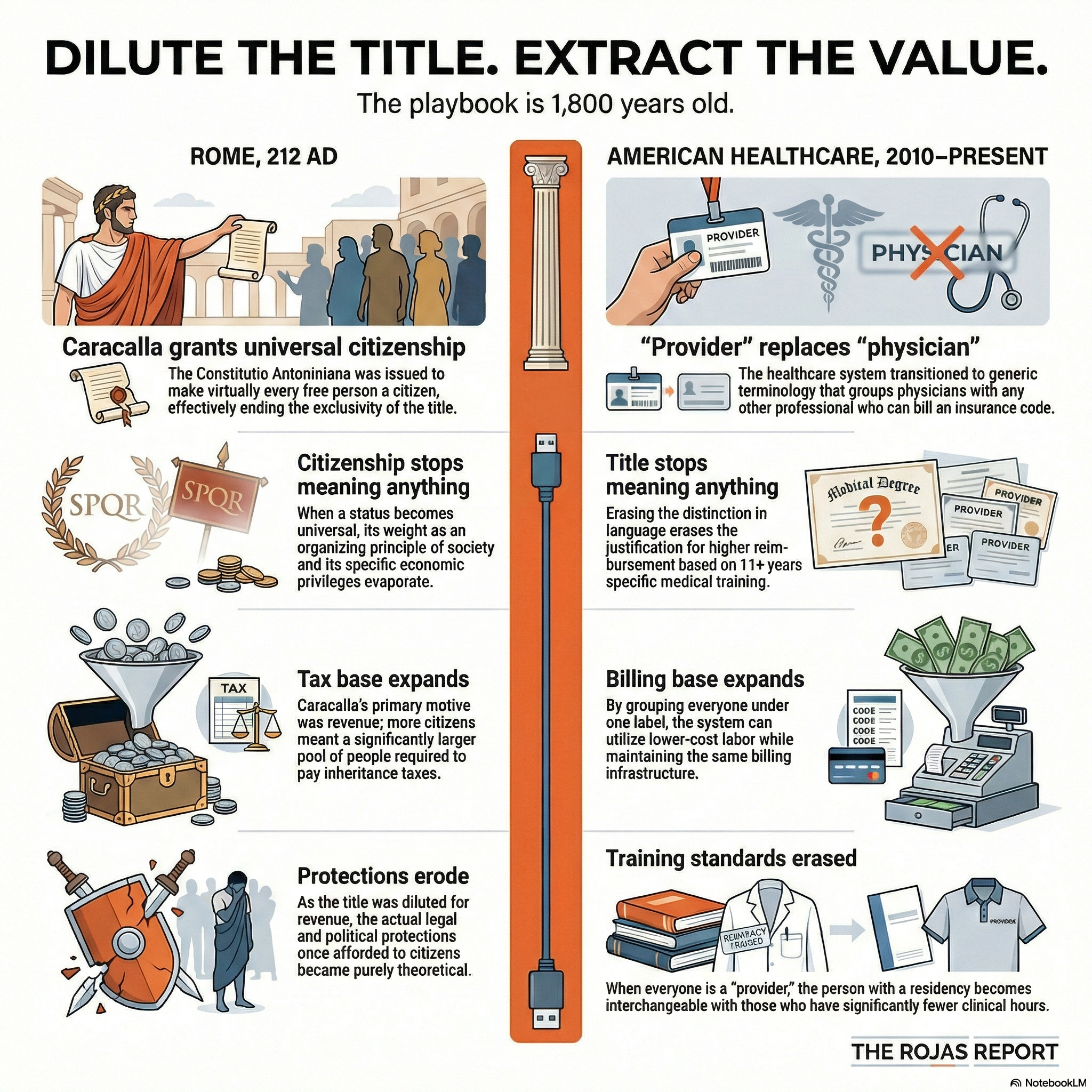
In 212 AD, Emperor Caracalla issued the Constitutio Antoniniana. It granted Roman citizenship to virtually every free person in the empire.
The history textbooks frame this as progressive.
Inclusive.
A broadening of rights.
It was a tax grab.
Roman citizenship had meant something specific. Legal protections. Political rights. Military obligations. Economic privileges. It was a status that carried weight because it was limited. Not everyone had it. The distinction mattered.
Caracalla didn’t care about rights. He cared about revenue. Citizens paid inheritance taxes. More citizens meant more tax revenue. So he diluted the title to expand the base.
The result was predictable. Citizenship stopped meaning anything. The legal protections eroded. The political rights became theoretical. The distinction between citizen and non-citizen, which had been the organizing principle of Roman society for centuries, evaporated.
He didn’t create more Romans.
He made “Roman” meaningless.
Now watch the same play in American healthcare.
The word “physician” used to mean something specific. Four years of medical school. Three to seven years of residency. Board certification. A defined scope of training that no other profession replicated.
Over the past two decades, the healthcare system systematically replaced “physician” with “provider.” A word that includes physicians, nurse practitioners, physician assistants, pharmacists, optometrists, chiropractors, and anyone else who can bill an insurance code.
Provider was never about access or approachability; it was about economics.
A physician costs more than a nurse practitioner. A nurse practitioner costs more than an imported physician. If you erase the distinction in language, you erase the distinction in reimbursement justification. If everyone is a “provider,” then the cheapest provider wins.
Caracalla didn’t grant citizenship to 30 million people.
He devalued what citizenship meant so he could extract more from it.
American healthcare didn’t expand access by calling everyone a “provider.” It devalued what “physician” meant, so it could pay less for it.
The play is 1,800 years old. It works every time. Because the propaganda that accompanies it is always the same: we’re not diluting. We’re including.
THE FOEDERATI BARGAIN
Rome’s military was the most expensive institution in the ancient world. Legionaries were professional soldiers. Career men. Trained, equipped, and paid by the state. The system worked as long as the money held.
When the money stopped holding, Rome made deals.
The foederati system was straightforward. Germanic tribes, including the Goths, Vandals, Franks, and others, were offered land, status, and payment in exchange for military service. They would guard Rome’s borders. Rome would keep the administrative structure. Everyone wins.
Except everyone didn’t win.
The foederati fought for pay, not for Rome. They had no institutional loyalty. They learned Roman tactics, Roman organization, and Roman vulnerabilities. And when the deals became unfavorable, they stopped pretending to be Roman.
The people Rome hired to defend the borders became the people who crossed them. American healthcare is running the same bargain.
The system can’t retain physicians. Burnout rates exceed 50% in some specialties. Administrative burden consumes roughly a quarter of practice revenue. Reimbursement rates decline in real terms every year. Independent practices close at a rate that would be called a crisis in any other industry.
So the system makes deals.
Locum tenens agencies. Travel nursing firms. Staffing companies that provide temporary clinical labor at premium rates to hospitals that have driven out their permanent physicians through administrative extraction.
Scope-of-practice expansion follows the same logic. If you can’t afford legions, hire mercenaries. If you can’t retain physicians, expand who counts as a physician.
And now there’s a new version of the play.
In 2025, North Carolina authorized a new license type allowing internationally trained physicians to practice in the state. No U.S. residency required. Virginia, Tennessee, and Florida passed similar laws. The stated goal: address physician shortages in rural and underserved areas.
The real math: a foreign-trained physician will work for less than $100,000. An American-trained physician with 11 years of training and six figures in medical school debt costs three to four times that. The hospital systems filling rural gaps aren’t recruiting American physicians at competitive salaries. They’re importing cheaper labor with provisional licenses and supervision requirements that keep the new hires dependent on the system.
This is the foederati bargain with a modern face. Rome didn’t recruit barbarians out of generosity. It recruited them because they were cheaper than legions. American healthcare isn’t licensing foreign physicians out of compassion. It’s licensing them because they cost less than the physicians the system drove out.
The issue is not nationality. It is structural arbitrage. When training standards, debt burdens, and licensing pathways vary widely, the system will exploit the lowest-cost configuration available. That is not a moral judgment. It is an economic one.
Scope expansion runs the same play from a different angle. Nurse practitioners get independent practice authority in a growing number of states. The training gap is measured in thousands of clinical hours. The billing codes are increasingly identical. Massage therapists bill insurance companies as “providers.” The word has been diluted so completely that it means anyone who submits a claim.
The foederati didn’t destroy Rome overnight. They replaced it gradually. One border post at a time. One garrison at a time. Until the thing that called itself the Roman military was mostly people who had never been Roman.
The “provider” model isn’t destroying medicine overnight. It’s replacing it gradually. One clinic at a time. One scope expansion at a time. Until the thing that calls itself healthcare is mostly made up of people who never completed a residency.
And the hospital systems brokering these deals will call it progress. Just like Rome called the foederati “allies.”
Rome called them allies.
Your hospital calls them “workforce solutions.”
The foederati bargain never ends well for the people being replaced.
60,000+ physicians are paying attention.
Subscribe
THE PROPAGANDA WAR
Empires don’t just fall. They narrate their own decline as progress.
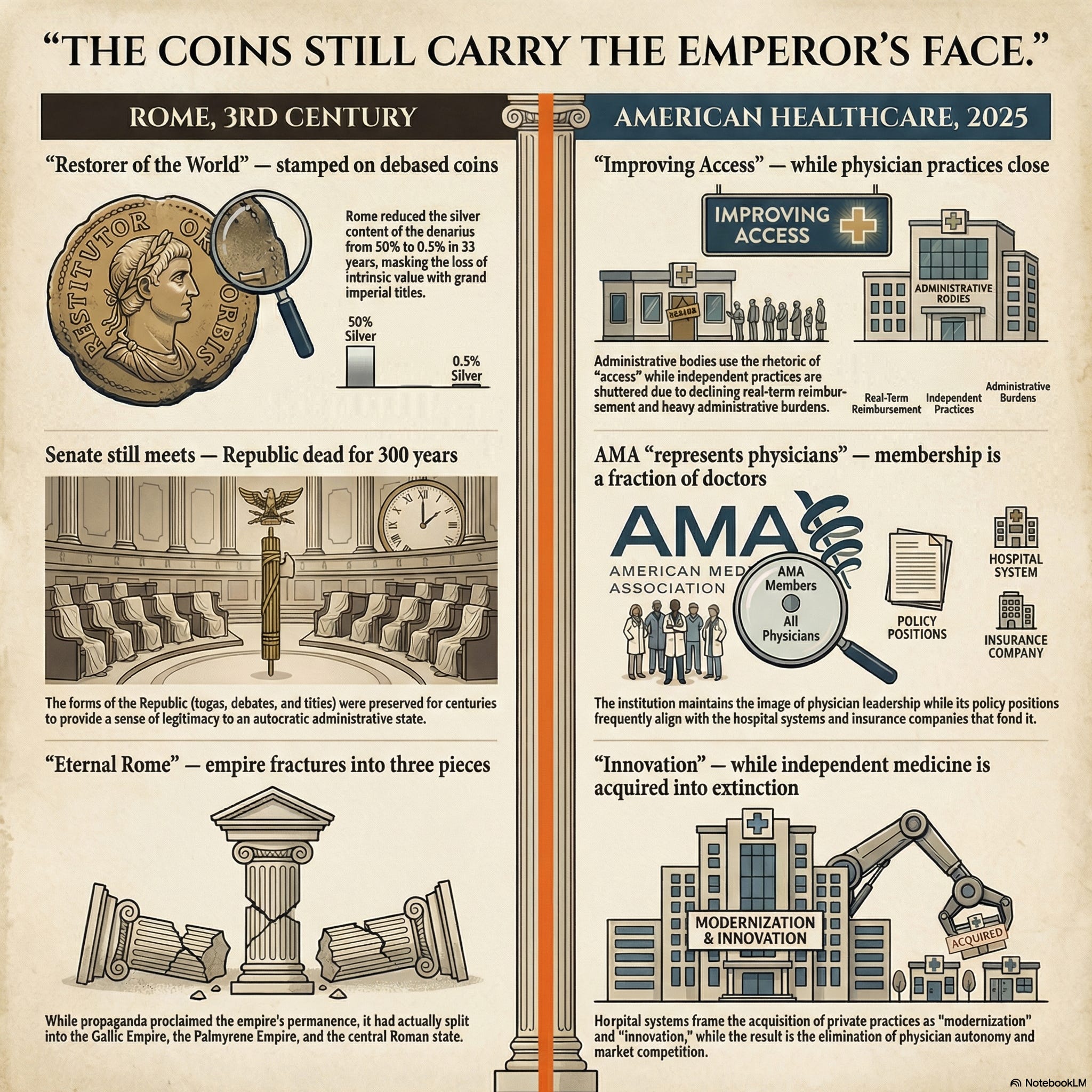
Rome’s coins in the 3rd century still carried the emperor’s face. Still bore inscriptions about “Restorer of the World” and “Eternal Rome.” The silver was gone. The title remained. The messaging machine ran at full capacity even as the thing it described was disintegrating.
The Senate still met. Senators still wore togas. Debates still happened. The forms of the Republic persisted for centuries after the Republic died. Because the forms were useful. They provided legitimacy. They made people believe the system was working even when their lived experience said otherwise.
American healthcare runs the same propaganda apparatus.
The AMA still claims to represent physicians. Its membership is a fraction of practicing doctors. (AMA Series) Its policy positions consistently favor the hospital systems and insurance companies that fund its operations. But the name carries weight. The institutional memory of what the AMA once was covers for what it actually does.
CMS frames every regulation as “improving access” and “ensuring quality.” Certificate of Need laws, which give existing hospitals veto power over new competitors, are framed as “preventing unnecessary duplication of services.” The language is always about the patient. The mechanism is always about the incumbent.
Hospital system press releases announce “expanded services” and “community partnerships” as they acquire independent practices, eliminate physician autonomy, and consolidate market power. The press release says “innovation.” The balance sheet says “extraction.”
Insurance companies run television ads about “caring for your health” while implementing prior authorization systems that delay care, deny claims, and shift costs to patients and physicians.
The coins still carry the emperor’s face.
The messaging is always the same: the system is working.
The system is improving.
The system cares about you.
If you’re a physician who has been through prior auth. If you’ve watched your reimbursement decline while your administrative burden doubled. If you’ve seen your colleagues leave medicine. If you’ve watched your practice get acquired by a system that promised partnership and delivered control.
You know.
Everyone knows.
The thing they keep describing no longer exists. What remains is the paperwork.
THE CURRENCY UNDERNEATH IT ALL
Every structural failure in both Rome and American healthcare connects back to money.
Rome debased the denarius from 50% silver to 0.5% in roughly 33 years. They couldn’t afford the legions, the grain dole, the bureaucracy, and the frontier defense simultaneously. So they shaved the coins. Printed money with less metal. Kept the image. Destroyed the value.
America runs the same play with more sophisticated tools.
The national debt sits at $38 trillion.
Annual interest payments hit $981 billion.
That’s nearly $1 trillion per year just to service existing debt.
Not to build anything.
Not to improve anything.
To pay interest on money already spent.
Healthcare spending reached $5.3 trillion in 2024. 18% of GDP. Growing at 7.2% per year, outpacing the GDP growth of 6%. CMS projects it will hit 20.3% of GDP by 2033.
The system’s commitments exceed its productive capacity. The gap gets filled by financial engineering. Deficit spending. Debt monetization. Medicare reimbursement rates decline in real terms while administrative costs compound. Medicaid programs that promise coverage while paying physicians below the cost of delivery.
Rome couldn’t afford legions, so it hired foederati. America can’t afford physicians, so it hires “providers.” Rome debased the currency to fund the gap. America monetizes debt to fund the gap.
The mechanism is more sophisticated.
The math is identical.
And just like Rome, the people at the top of the system don’t experience the debasement. Senators in Rome still lived well in the 3rd century. Hospital system CEOs pulling $5 million, $10 million, $20 million in compensation don’t experience the physician shortage. The extraction machine works perfectly for the people running it.
It only breaks for everyone else.
Medicare reimbursement is not set in isolation. It exists inside federal fiscal constraint. When annual interest approaches $1 trillion, discretionary expansion becomes politically implausible. Medicare sets the benchmark. Commercial insurers anchor to Medicare multiples. When explicit rationing is politically toxic, rationing shifts into complexity. Administrative burden becomes the substitute for overt price control. That burden lands on physicians.
1913: THE YEAR AMERICA CHANGED OPERATING SYSTEMS
Rome’s structural collapse played out over decades. America’s played out in a single calendar year.
November 1910. Six men board a private railcar in New Jersey under the cover of a duck hunting trip. Senator Nelson Aldrich, Republican whip in the Senate, chairman of the National Monetary Commission, Rockefeller’s father-in-law. Henry P. Davison, J.P. Morgan’s partner. Paul Warburg, Kuhn Loeb partner. Frank Vanderlip, president of Rockefeller’s National City Bank. Charles Norton, president of Morgan’s First National Bank. A. Piatt Andrew, Assistant Secretary of the Treasury.
They travel to the Jekyll Island Club off the coast of Georgia. Membership included Morgan, Rockefeller, and Vanderbilt. Munsey’s Magazine called it “the richest, the most exclusive, the most inaccessible” club in the world.
For nine days, they draft the framework for a central banking system.
The participants denied the meeting happened for twenty years.
Frank Vanderlip later wrote that the secret expedition to Jekyll Island was “the actual conception of what eventually became the Federal Reserve System.” He also admitted he had been “as secretive, indeed, as furtive, as any conspirator.”
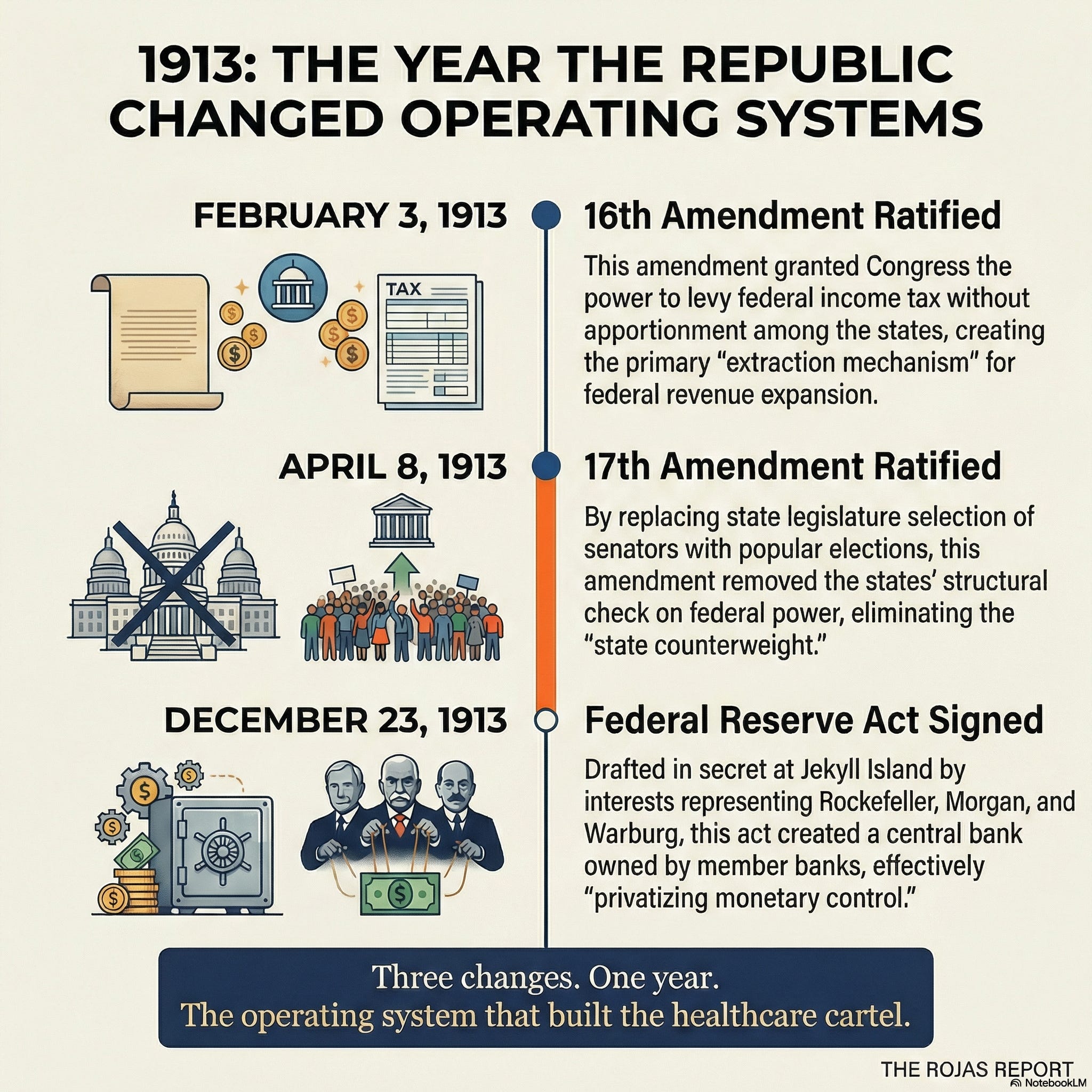
On December 23, 1913, the Federal Reserve Act became law. A central banking system that blended public authority with private balance sheets. Structurally independent. Operationally insulated. Democratically distant. Designed to expand monetary elasticity without expanding electoral accountability. A. Barton Hepburn told the American Bankers Association that same year: the new system “recognizes and adopts the principles of a central bank” and would “make all incorporated banks together joint owners of a central dominating power.”
Rome outsourced its military to the foederati. America outsourced its monetary system to the banking families who drafted the legislation on a private island.
But 1913 didn’t stop there.
February 3, 1913. The 16th Amendment is ratified. Congress gains the power to levy income tax on individuals without apportioning it among the states. In its first year, less than 1% of the population paid income tax, at a rate of 1%. The mechanism was small. The precedent was total. The extraction apparatus had its power source.
April 8, 1913. The 17th Amendment is ratified. Senators, previously selected by state legislatures, are now elected by popular vote.
This is the one that doesn’t get enough attention.
The Founders’ design was specific. The House represented individuals. The Senate represented states as sovereign entities. State legislatures picked their senators, which meant states had a direct structural check on federal power. If Washington overreached, the states had a seat at the table to push back.
The 17th Amendment removed that seat.
James Madison argued that the arrangement would serve as a “convenient link” between the two systems and protect against “improper acts of legislation.” The original design created two chambers drawn from different constituencies, different incentive structures, different loyalties. Even the Anti-Federalists who feared the Senate’s power, George Mason among them, understood that the selection mechanism mattered. Mason refused to sign the Constitution in part because he feared the Senate would become an unaccountable aristocracy. But even Mason’s critique assumed senators would answer to state legislatures, not to popular mobs and party machines. The 17th removed the structural tension entirely.
The 17th turned the Senate into a second House. Popular election means senators answer to voters, donors, and party machinery. Not to the state governments that were supposed to serve as the counterweight to centralization. The structural brake on federal expansion was removed.
Three changes. One year.
1913 did not predetermine the healthcare cartel. It made it structurally feasible. It expanded federal revenue capacity, weakened state counterweights, and insulated monetary elasticity from direct democratic pressure. What followed was not inevitable. It was enabled.
The extraction mechanism (income tax). The removal of state-level resistance (popular Senate elections). The privatization of monetary control (the Federal Reserve).
Caracalla diluted citizenship to expand his tax base. America expanded the tax base, removed the states’ check on it, and handed monetary policy to the people who would profit from it. Same playbook. Better execution.
The pre-1913 republic was not a golden age. It had corruption, instability, and regional inequities. The New Deal built real safety nets. The administrative state solved real crises. The question is not whether these reforms addressed problems. The question is what incentive structures they permanently embedded.
Then came the man who used the new operating system to its full capacity.
Franklin Roosevelt issued 3,725 executive orders. More than any president in American history, by a factor of three. The National Industrial Recovery Act alone allowed Roosevelt to allocate $3.3 billion without congressional approval. At least 69 new federal agencies were created during the New Deal. Al Smith, a fellow Democrat who turned against Roosevelt, said his government was “submerged in a bowl of alphabet soup.” Even the Comptroller General of the United States admitted he had never heard of some of them.
The administrative state didn’t grow. It was manufactured.
Roosevelt didn’t break the republic’s design. The design was already broken. 1913 removed the structural limits. FDR operated within the new parameters. Executive orders became a governing mechanism, not an exception. The alphabet agencies created a permanent bureaucratic infrastructure that outlived the crisis they were built to address. The SEC. The FHA. The FDIC. Social Security. Emergency measures that became the permanent architecture of federal power.
Diocletian didn’t restore the Roman Republic. He built a new operating system. More centralized. More bureaucratic. More expensive. More authoritarian. The version of Rome that survived the Crisis of the Third Century looked nothing like the version that entered it.
FDR didn’t restore the American republic as designed. He built a new operating system on the foundation that 1913 made possible. More centralized. More bureaucratic. More expensive. The version of American government that emerged from the New Deal and World War II looked nothing like the version the Founders designed.
The coins still carried the eagle. The title still said “Republic.” The operating system was something else entirely.
And that operating system is what built the healthcare cartel.
Medicare. Medicaid. Certificate of Need. The Hill-Burton Act’s transformation from a construction program into a regulatory apparatus. The entire framework that allows hospital systems to operate as tax-exempt monopolies while extracting $5.3 trillion per year from the economy. None of it is possible without the federal infrastructure that 1913 enabled, and FDR built.
The Founders designed hardware: divided sovereignty, state representation, and limited federal reach. 1913 rewrote the firmware: revenue expansion, centralized monetary elasticity, weakened state resistance. FDR installed applications that could not be uninstalled.
The healthcare cartel didn’t capture a functioning republic. It captured an administrative state that was already designed for capture.
The operating system was rewired in 1913.
The healthcare cartel was built on top of it.
Physicians who understand the architecture are the ones who will build what replaces it. 60,000+ are already here.
THE QUESTION THAT DECIDES EVERYTHING
Rome survived the Crisis of the Third Century. Aurelian reunified the empire by force. Diocletian rebuilt it from scratch. New tax system. New administrative structure. New military organization.
But the thing that survived was unrecognizable. More authoritarian. More bureaucratic. More expensive. More centralized. The Roman people's romanticization was already dead. What replaced it was a control structure designed to prevent the next collapse, not to restore what was lost.
American healthcare faces the same fork.
If physicians wait for the institutions to reform, they’ll get the Diocletian solution. More centralization. More bureaucracy. More cost. Government-run systems that eliminate the dysfunction by eliminating the autonomy. The hospital cartel was replaced by a federal cartel. Different flag. Same extraction.
If physicians build now, they write the terms of what comes next.
Independent infrastructure. Shared services. Collective bargaining power outside the hospital system. Administrative platforms that provide what hospital systems hold over physicians’ heads: benefits, insurance, payroll, compliance, HR, and retirement. Not because the old system will graciously step aside. It won’t. Rome’s institutions didn’t voluntarily cede power.
They were made irrelevant by better structures.
Diocletian didn’t ask the Praetorian Guard for permission to reorganize the military.
Physicians don’t need to ask the hospital cartel for permission to reorganize medicine.
The ending of this story isn’t written yet.
History doesn’t repeat. But the structural patterns do. Currency debasement. Title dilution. Outsourced defense. Propaganda masking decline. Regional fracturing. Institutional capture. And in America’s case, a single year that rewired the republic’s operating system to enable all of it.
Rome ran that sequence for over 50 years.
American healthcare is running it now.
By the time Diocletian stabilized Rome, no one remembered what the Republic felt like. Stability replaced liberty. Administration replaced citizenship. Order replaced ownership. The empire survived. The republic did not.
The people who build what comes next will define what survives.
-Rojas out.
WORK WITH DUTCH
This article describes the problem. These are the things I’m working on to fix them.
The Rojas Report produces daily media that teaches the American people how the U.S. healthcare system actually works. Who profits. Who pays. Who decides. You’re reading it.
MedMerge builds economic infrastructure for independent medical practices. Benefits, insurance, artificial intelligence layers, and shared services. Fortune 500-level coordination without ownership transfer. The advantages hospital systems have over independent physicians stem from scale. MedMerge provides the scale without the surrender.
PhyCap Fund invests in physician-led healthcare startups. Venture capital by physicians, for physicians. The capital formation layer that turns independent medicine from a defensive position into an offensive one.
PHA (Physician-Led Healthcare for America) lobbies to protect and expand the independent practice of medicine. Policy. Legislation. State-level fights. The political arm of a movement that refuses to wait for the cartel to reform itself.
The article you just read explains why the system was built for capture.
These four organizations are what capture-proof infrastructure looks like.
GLOSSARY
Pax Romana: Latin for “Roman Peace.” Roughly 200 years (27 BC to 180 AD) of relative stability across the Roman Empire. Institutions were strong enough to absorb bad emperors without systemic collapse. The healthcare equivalent: post-WWII American medicine, when physicians ran independent practices and hospitals were community institutions.
Crisis of the Third Century: The 50-year period (235-284 AD) during which Rome cycled through 20+ emperors, the currency was debased to worthlessness, and the empire fractured into three competing states. If you were alive during this, your world was falling apart.
Postumus: Military commander who declared himself emperor of the Gallic Empire in 260 AD. Took Gaul, Britannia, and Hispania. Not through conquest. Through competence. He delivered what Rome couldn’t. The healthcare equivalent: states that build their own regulatory frameworks because the federal system stopped functioning.
Zenobia: Queen of Palmyra who took control of Rome’s eastern provinces including Syria, Egypt, and parts of Asia Minor. Built a competing power structure because the center couldn’t hold. The healthcare equivalent: regional health systems and physician networks that operate independently of federal oversight in practice if not in name.
Constitutio Antoniniana (212 AD): Caracalla’s edict granting Roman citizenship to virtually all free persons in the empire. Framed as inclusion. Functioned as a tax grab. Diluted what citizenship meant so more people could be taxed. The healthcare equivalent: replacing “physician” with “provider” to expand the billing base while erasing the training distinction.
Foederati: Barbarian tribes hired by Rome to guard its borders because Rome couldn’t afford its own legions. They learned Roman tactics, held Roman positions, and eventually replaced the system they were hired to defend. The healthcare equivalent: locum tenens agencies, travel nursing firms, and scope-expanded non-physician clinicians filling gaps created by a system that drove physicians out.
Denarius: Rome’s standard silver coin. Went from 50% silver to 0.5% in roughly 33 years. The coin looked the same. The value was gone. The healthcare equivalent: your insurance card still looks like insurance. The coverage behind it buys less every year.
Jekyll Island (1910): The secret meeting of six men representing the Rockefeller, Morgan, and Warburg banking interests at a private resort off the Georgia coast. They drafted the framework for the Federal Reserve Act under the cover of a duck hunting trip. The participants denied the meeting occurred for twenty years. The healthcare equivalent: Certificate of Need boards where hospital executives meet behind closed doors to decide whether competitors can exist.
16th Amendment (1913): Constitutional amendment granting Congress the power to levy income tax on individuals without apportioning it among the states. Created the federal extraction mechanism. In its first year, less than 1% of the population paid, at a rate of 1%. The mechanism was small. The precedent was total.
17th Amendment (1913): Constitutional amendment replacing state legislature selection of senators with popular election. Removed the states’ structural check on federal power. The Founders designed the Senate to represent states as sovereign entities. The 17th turned it into a second popularity contest. The healthcare equivalent: when the AMA stopped representing physicians and started representing the institutions that fund it.
Diocletian: Roman emperor (284-305 AD) who ended the Crisis by replacing the entire operating model. Didn’t reform the old system. Built a new one. The version of Rome that survived looked nothing like the version that entered the crisis.
Certificate of Need (CON): State laws requiring anyone building a new healthcare facility to prove “need.” In 35 states, existing hospitals decide whether competitors can exist. The Praetorian Guard picks the next emperor.
Currency Debasement: Reducing the intrinsic value of money while maintaining its face value. Rome shaved the silver. America monetizes debt. The mechanism evolves. The math doesn’t.
SOURCES
Health Affairs Journal, “National Health Care Spending Increased 7.2 Percent In 2024,” January 2026. US healthcare spending reached $5.3 trillion in 2024, 18% of GDP.
Health Affairs Journal, “National Health Expenditure Projections, 2024-33.” Projects healthcare reaching 20.3% of GDP by 2033.
U.S. Congress Joint Economic Committee, Monthly Debt Update, December 2025. National debt at $38.40 trillion, annual interest payments at $981 billion.
Committee for a Responsible Federal Budget, “Gross National Debt Reaches $38 Trillion,” October 2025.
CMS National Health Expenditure Data, historical (1960-2023). 2001 spending: approximately $1.4 trillion, 13.3% of GDP.
Peterson-KFF Health System Tracker, “How Much Is Health Spending Expected to Grow?” August 2025. Hospital spending estimated at $1.8 trillion in 2025.
Congressional Budget Office, Federal Debt and the Debt Limit in 2025. Total federal debt at $37.6 trillion at end of FY2025, 122.6% of GDP.
National Archives, “16th Amendment to the U.S. Constitution: Federal Income Tax (1913).” Ratified February 3, 1913. Less than 1% of the population paid income taxes at the rate of only 1% of net income.
National Archives, “17th Amendment to the U.S. Constitution: Direct Election of U.S. Senators (1913).” Ratified April 8, 1913.
U.S. Senate Historical Office, “Landmark Legislation: The Seventeenth Amendment to the Constitution.”
Federal Reserve History, “The Meeting at Jekyll Island.” Six participants; meeting denied for twenty years; Aldrich Plan became basis for Federal Reserve Act.
Richmond Federal Reserve, “Jekyll Island: Where the Fed Began,” 2015. Munsey’s Magazine “richest, most exclusive, most inaccessible” club description.
Wikipedia, “List of Executive Actions by Franklin D. Roosevelt.” 3,725 executive orders, numbered 6071-9537. Highest of any single president by a factor of three.
Wikipedia, “Alphabet Agencies.” National Industrial Recovery Act allowed $3.3 billion allocation without Congress; Al Smith “alphabet soup” quote; Comptroller General quote.
Vanderlip, Frank A. “From Farm Boy to Financier,” Saturday Evening Post, February 9, 1935. “As secretive, indeed, as furtive, as any conspirator” and “actual conception” quotes.
Hepburn, A. Barton. Address to American Bankers Association, August 1913. “Joint owners of a central dominating power” quote.
Cassius Dio, Roman History, Book 78. Caracalla and the Constitutio Antoniniana (212 AD).
Harl, Kenneth W. Coinage in the Roman Economy, 300 B.C. to A.D. 700. Johns Hopkins University Press, 1996. Roman denarius silver content decline.
Drinkwater, J.F. The Gallic Empire: Separatism and Continuity in the North-Western Provinces of the Roman Empire, A.D. 260-274. Franz Steiner Verlag, 1987.
Stoneman, Richard. Palmyra and Its Empire: Zenobia’s Revolt Against Rome. University of Michigan Press, 1992.
Heather, Peter. The Fall of the Roman Empire: A New History of Rome and the Barbarians. Oxford University Press, 2006.
National Conference of State Legislatures, Certificate of Need State Laws database.
Medscape, National Physician Burnout and Suicide Report, 2024.
American Association of Nurse Practitioners, State Practice Environment map, 2025.
North Carolina Medical Board, new license type for internationally trained physicians, authorized by 2025 state law. Similar laws in Virginia, Tennessee, and Florida. KFF Health News, NPR reporting.