The 145% Markup: Why Catholic Systems Are Buying Your Practice
Dynasty 3: The Cross-Market Consolidators

They’re not buying your practice because they need doctors.
They’re buying it to exploit a payment loophole where Medicare reimburses 50–145% more for procedures when you’re hospital-owned.
Same colonoscopy.
Same you.
Same room.
In many markets,
reimbursement more than doubles after conversion.
That’s the facility fee.
That’s the game.
The Math
Here’s how it works.
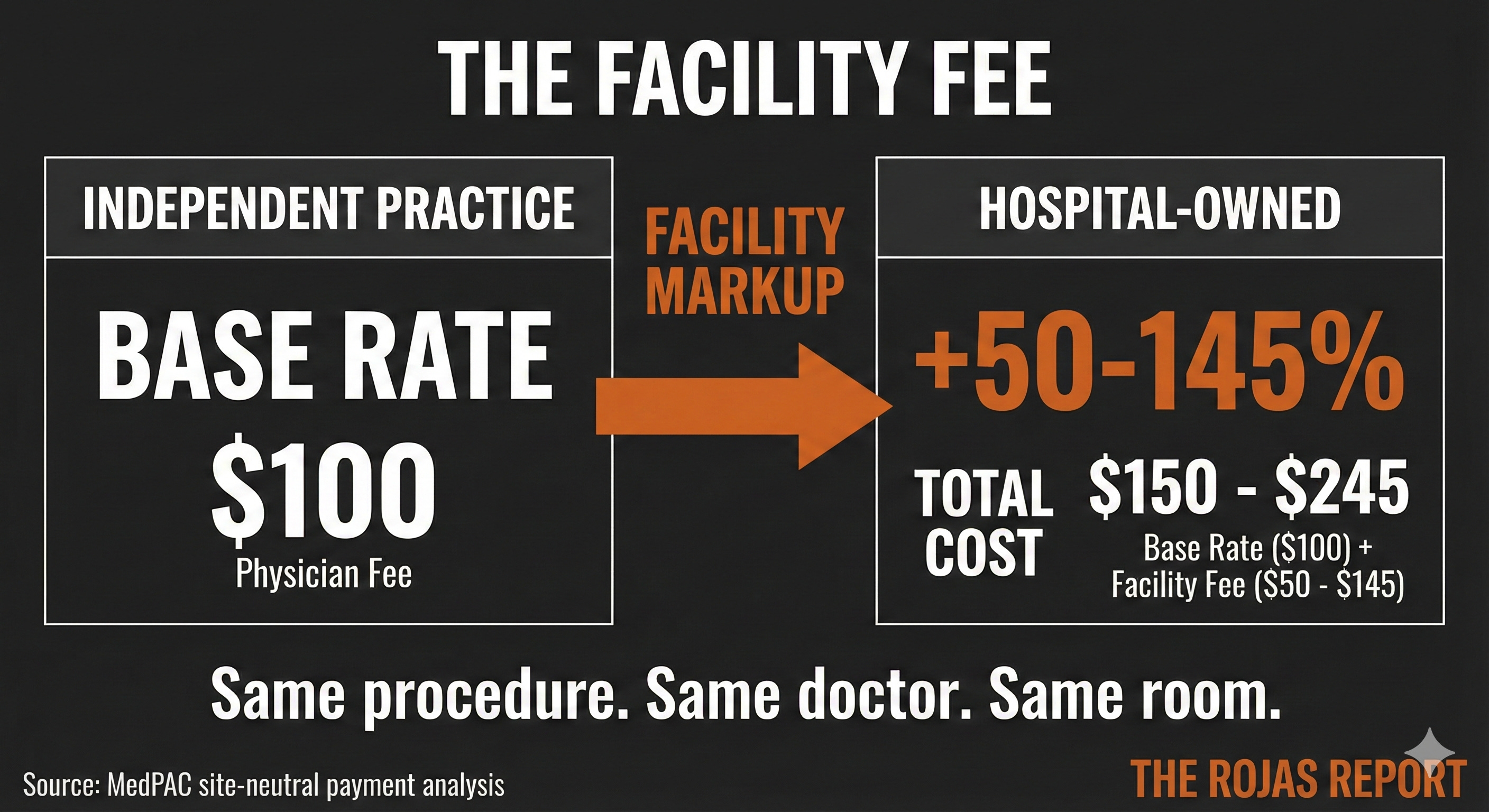
You perform a colonoscopy in your independent practice. Medicare pays one rate.
A Catholic system buys your practice.
Converts it to a hospital outpatient department.
You perform the same colonoscopy.
Same scope. Same hands. Same recovery room.
Medicare pays 50-145% more, depending on the service and the market.
For a typical Medicare patient undergoing a colonoscopy, this increase could translate into several hundred dollars more in out-of-pocket expenses. The difference is a facility fee, a billing code that exists because you’re now hospital-owned. This code is activated under current CMS rules, which recognize hospital ownership as a trigger for higher reimbursement rates due to assumed facility costs.
You didn’t get better.
The procedure didn’t change.
The patient didn’t benefit.
In fact, the patient often pays a higher coinsurance amount.
Dr. Cohen, a gastroenterologist, recalls the day when her thriving independent practice was purchased by a Catholic system. The promise of streamlined resources and increased reach seemed enticing, but reality soon set in. She conducted a colonoscopy, as she had done countless times before. Same equipment, same office, yet this time, the bill sent to Medicare was substantially higher. Patients started noticing the difference too, complaining about the unexpected jump in their out-of-pocket expenses.
But the bill went up. MedPAC has documented this for years. They’ve repeatedly recommended site-neutral payment reform precisely because of this abuse. Multiply that by every patient. Every procedure. Every acquired physician.
Now you understand why they paid 3x your billings to buy you.
The Scale
You’re not alone.
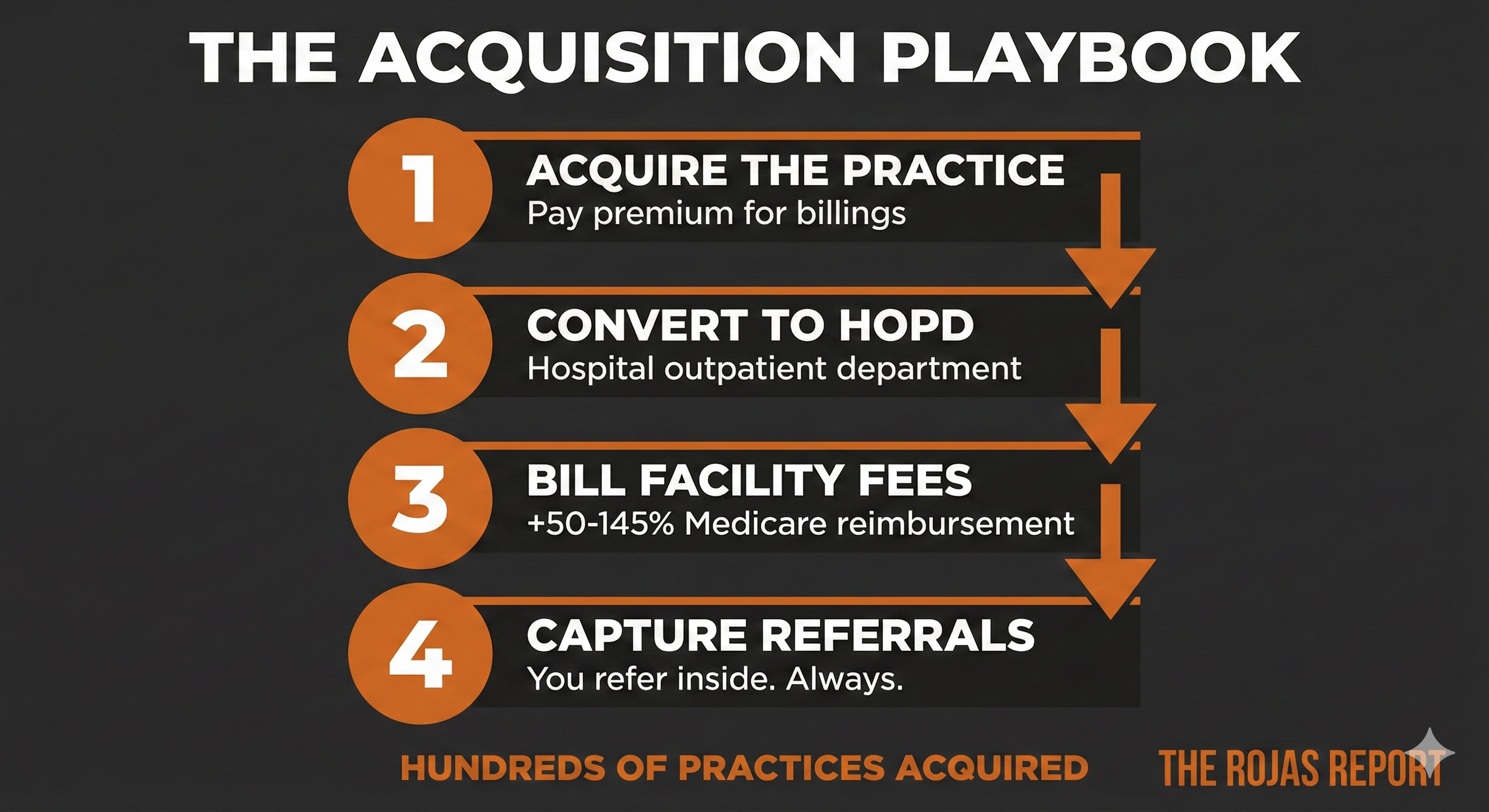
The top Catholic systems have acquired hundreds of physician practices and clinics.
They’re not building.
They’re buying.
And every acquisition follows the same playbook:
Acquire the practice and convert it to a hospital outpatient department. This allows facility fees to be billed on every visit, maximizing revenue potential.
Capture the referral network.
Once you’re inside, you refer inside.
Your patients go to their imaging centers.
Their surgery centers.
Their hospitals.
You’re not a physician anymore.
You’re a revenue engine with a white coat.
Estimated incremental facility-fee revenue across six Catholic systems: $2-5 billion annually.
The Moat
Why can’t anyone compete this away?
Because Catholic systems have built regulatory walls that no one can climb.
Certificate of Need laws (state permits that limit new competitors). 34 states and Washington D.C. require government approval to open a new hospital or add services. Incumbent hospitals can object. And they do.
Catholic systems operate overwhelmingly in CON states:
CommonSpirit: 86% of states have CON laws
Ascension: 79%
Trinity: 82%
Bon Secours: 86%
No new hospital can open to compete, and no new surgery center can offer lower prices. The market is frozen by law. In practice, this frozen market often results in significantly higher local insurance premiums and longer travel distances for those in need of affordable care.
For instance, some rural areas report that residents must travel over 50 miles for competitive services, adding substantial time and travel expenses to already costly healthcare needs.
Cross-market mergers.
The FTC reviews mergers for competitive harm. But they define markets geographically.
So when Dignity (California) merged with CHI (Midwest) to form CommonSpirit, no FTC challenge. Different geographies. No “local” overlap.
Catholic systems built national empires through mergers that the FTC couldn’t touch.
Church plan exemption.
Catholic systems claim an exemption from ERISA, the federal law that protects workers’ pensions.
No Pension Benefit Guaranty Corporation (PBGC) insurance.
No federal oversight.
No minimum funding standards.
Ascension settled a $90 million pension underfunding case in 2016.
Trinity settled for $75 million in 2019.
St. Clare’s Hospital in New Jersey went bankrupt, 700 retirees lost everything.
1 million+ healthcare workers have no federal pension protection because their employer claims to be a church.
The Money Trail
Where does it go?
Not to charity care. Catholic hospitals provide only 2.7% of expenses as charity care, which falls below the national average of 3.87%. This is in stark contrast to the mission statement of many Catholic systems, which often emphasize community service and care for the needy. For instance, CommonSpirit Health states as part of its mission, “to provide quality, compassionate care to the communities we serve.” Juxtaposed with the 2.7% charity care figure, it raises questions about priorities and accountability.
Not to the community. Five Catholic systems have a combined fair-share deficit of $3.8 billion, meaning they receive $3.8 billion more in tax breaks than they pay in taxes.
Fair Share Deficit:
Providence-$1.0 billion
CommonSpirit-$923 million
Trinity-$784 million
Ascension-$614 million
Bon Secours Mercy-$488 million
Five of the ten worst fair share deficits in the country are all Catholic systems.
So where does it go?
Executive compensation.
CommonSpirit CEO:
2020:$16.7 million
2021: $14.6 million
2022: $35.5 million
*2023: $28.0 million
*That 2023 number,
including deferred compensation and severance tied to his final year.
10 CommonSpirit executives took home $94 million from 2020 to 2023.
Ministry on the letterhead.
Private equity math in the boardroom.
The Tax Advantage
Catholic systems don’t compete on the same playing field.
Estimated annual tax advantage (6 systems):
Annual Savings:
Federal income tax: $1.0 billion
State income tax: $300 million
Property tax: $500 million
Sales tax: $100 million
Total: $1.9 billion annually
For-profit hospitals pay 21% federal tax. Catholic systems pay zero.
For-profit hospitals pay property taxes on every building. Catholic systems pay zero.
Cumulative advantage over 10 years: $19 billion.
Add the combined subsidy exposure:
340B drug revenue $5-10 billion
DSH/UPL payments $3-5 billion
GME funding $1.3 billion
Facility fees $2-5 billion
Total $11-21 billion annually.
This range spans a conservative estimate for 340B drug revenue and an upper bound for potential DSH/UPL payments, ensuring clarity in understanding the nature and potential variance of these figures.
They’re playing a different game with different rules.
And they wrote the rules.
The 688
Here’s where it gets personal.
688 communities in America have only a Catholic hospital.
No alternative.
No competition.
No choice.
If you’re a physician in one of those communities, you have one employer.
If you’re a patient, you have one option.
And that option follows the Ethical and Religious Directives issued by the U.S. Conference of Catholic Bishops.
Prohibited services:
Sterilization (tubal ligation, vasectomy)
Contraception
IVF and fertility treatment
Death with dignity
If you’re an OB/GYN in one of those 688 communities, you practice medicine with a bishop looking over your shoulder.
If you’re a woman having a miscarriage in one of those 688 communities, you may be transferred to another hospital, if there is one.
CON laws keep it this way. No new hospital can open. The monopoly is protected by law.
The Acquisition Pipeline
They’re not slowing down.
CommonSpirit (2024): Acquired four hospitals and 35+ clinics from Steward Health Care in Utah.
Trinity (2024): Acquired CommonSpirit’s share of MercyOne Health System, expanding footprint across Iowa and the Midwest.
Ascension (2024): Divested Illinois hospitals to Prime Healthcare while expanding ambulatory footprint in core markets.
More practices. More facility fees. More market power.
The consolidation continues.
The Bottom Line
They’re not buying your practice because they need doctors.
They’re buying your practice because Medicare pays 50–145% more when you’re hospital-owned.
They’re protected by CON laws that block competition.
They’re shielded by cross-market merger loopholes the FTC can’t touch.
They’re exempt from pension laws that protect every other worker.
They provide less charity care than secular hospitals.
They pay executives $28 million, including deferred comp and severance.
And they call it ministry.
Tomorrow: Dynasty 4
The Regional Monopolies: UPMC, Sutter, Intermountain, Advocate, Geisinger.
They built their own health plans.
They went to war with insurers.
They won.
Now they control the beds AND the premiums.
The Five Dynasties Series
Kaiser: The Integration Template
Academic Medical Centers: The Prestige Cartel
Catholic Systems: The Cross-Market Consolidators ← You are here
Regional Monopolies: The Payer-Provider Fortresses
340B Empires: The Safety-Net Exploiters.
Your support funds the journalism they don’t want published.
Dutch Rojas is a healthcare entrepreneur and the publisher of The Rojas Report. He is the author of Too Big To Care: How Nonprofit Health Systems Hijacked Healthcare.
-Rojas out