
The Five Dynasties of Healthcare
The Nonprofit Architects Who Built the Castle the Five Families Inherited

You know the Five Families.
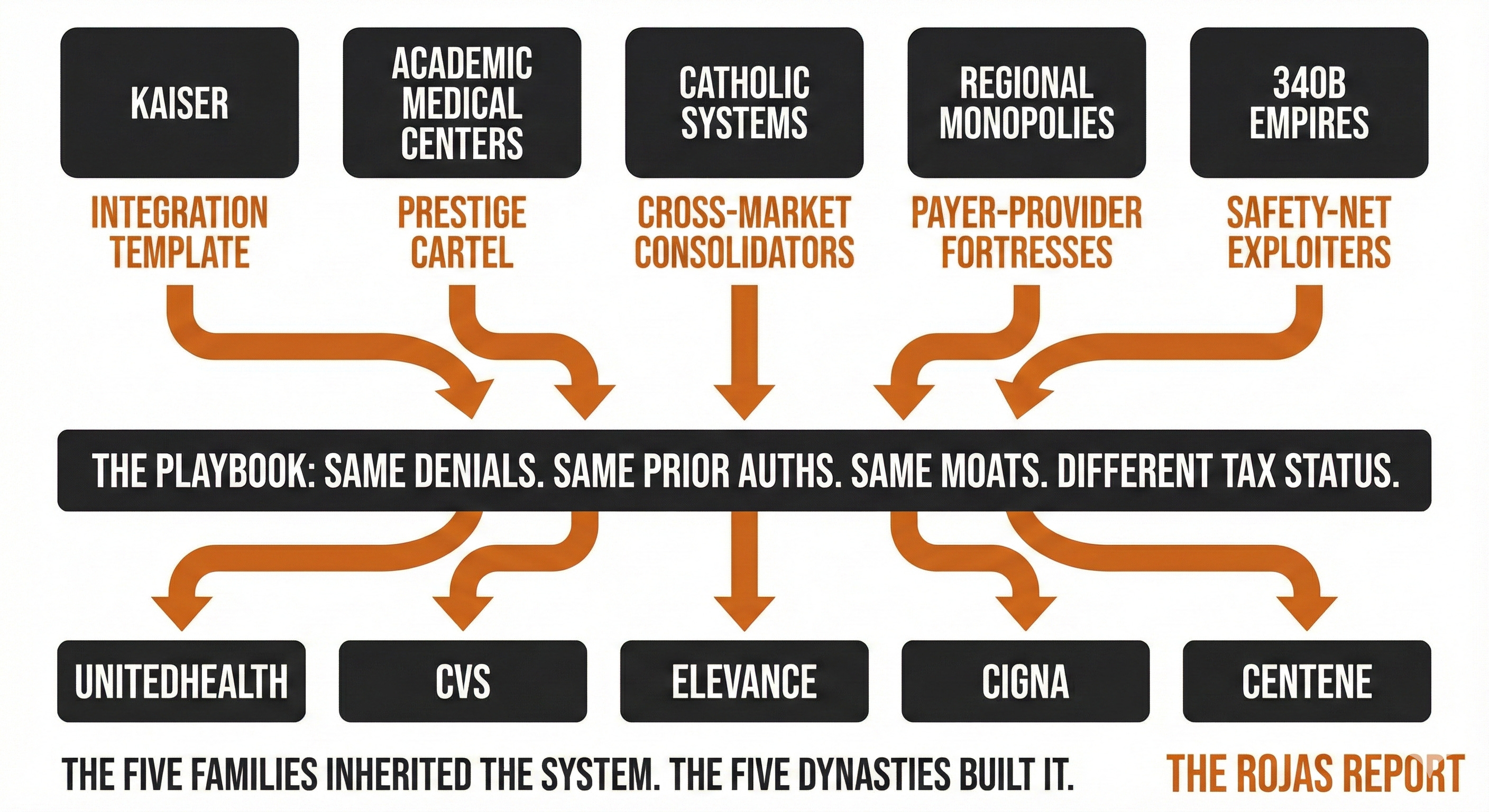
UnitedHealth. CVS. Elevance. Cigna. Centene.
The for-profit giants everyone loves to hate.
The publicly traded villains.
The ones whose denials make the news.
Yet there is a secret that 99.9% of the American populations does not know and I am going to reveal it to you today.
The 5 families didn’t build this system.
They inherited it.
The Dynasties Came First
Before the Five Families consolidated insurance, five nonprofit dynasties built the moats that make American healthcare unassailable.
They captured the regulations.
They wrote the rules.
They stacked advantages that their competitors can’t access.
And they did it while calling themselves charities.
The Five Families looked at what the Dynasties had built and said, “We can do that too.”
The difference? The Families are visible. The Dynasties kept their reputation.
The Five Dynasties
Dynasty 1: Kaiser: The Integration Template
Kaiser Permanente proved the model.
Own the insurance. Own the doctors. Own the hospitals. Control the entire flow of care from premium to prescription.
12.6 million members. Over $100 billion in annual revenue. A closed system where the payer and the provider are the same entity.
When Kaiser denies a claim, there’s no external insurer to blame. The denial comes from inside the house.
Kaiser showed that integrated nonprofits will manage utilization just like for-profit insurers do. They call it “coordinated care” instead of “prior authorization.”
The Five Families studied this model carefully.
Optum didn’t grow to 90,000 physicians by accident. They were copying Kaiser’s homework.
Dynasty 2: Academic Medical Centers: The Prestige Cartel
Hopkins. Penn. Duke. Yale. NYU. UPMC. Cleveland Clinic. Vanderbilt.
The academic medical centers built a fortress out of prestige — and then weaponized it.
Their moats:
GME Funding: Medicare pays over $16 billion annually for Graduate Medical Education, AMCs control who becomes a doctor. Residency slots have been capped since 1997. The physician shortage is a feature, not a bug.
CON Protection: In 34 states + Washington D.C., you can’t build a competing hospital without permission from the incumbents. The AMCs sit on the boards that decide.
NIH Funding: Billions in federal research dollars flow to academic centers. Taxpayer-funded research becomes privately profitable through the Bayh-Dole Act.
340B Eligibility: AMCs qualify for steep discounts on drugs. Buy low, bill high, keep the spread.
Facility Fees: When an AMC acquires a physician practice, Medicare pays 40-100% more for the same service. Same doctor. Same stethoscope. Different building.
AMCs charge 47% more than community hospitals for the same procedures. Not because outcomes are always better. Because they can.
The prestige justifies the pricing. The data often doesn’t.
Dynasty 3: Catholic Systems: The Cross-Market Consolidators
CommonSpirit. Ascension. Providence. Trinity. Bon Secours Mercy.
More than half of the ten largest health systems in America are Catholic-affiliated. They speak the language of ministry and community benefit.
The numbers tell a different story.
Fair Share Deficits: Five of the ten health systems with the most significant gaps between tax breaks received and charity care provided are Catholic. Providence, CommonSpirit, Trinity, Ascension, and Bon Secours Mercy each reported deficits of $488 million to $1 billion.
Executive Compensation: CommonSpirit’s CEO earned $28 million in 2022. Ministry on the letterhead. Private equity math in the boardroom.
COVID Relief: Ascension took $211 million in COVID relief while sitting on $15.5 billion in cash reserves — enough to operate for eight months without revenue.
Cross-Market Mergers: Catholic systems grew by combining hospitals in different geographies rather than in the same city. These deals are harder for the FTC to challenge, even though research shows they raise prices just the same.
And some operate health plans—same denials. Same prior auths, just with a crucifix in the lobby.
Dynasty 4: Regional Nonprofit Monopolies: The Payer-Provider Fortresses
UPMC is the archetype.
In the 1990s, the University of Pittsburgh Medical Center looked at its market and realized something no one else would say out loud: if you’re the dominant hospital system, why are you paying an insurance company to manage your patients?
So they built their own health plan. Then they went to war with Highmark, the region’s dominant Blue Cross insurer.
UPMC announced it would stop accepting Highmark patients. The state intervened. There were lawsuits, consent decrees, and years of chaos for patients caught in the middle.
UPMC won. They are now the largest insurer in Western Pennsylvania. They control the beds and the premiums. The employer must offer a plan that includes UPMC, meaning the employer must offer the UPMC plan.
This is the Kaiser model, but without the nonprofit halo. UPMC understood that integration isn’t about efficiency. It’s about leverage.
Sutter in California. Intermountain in Utah. Advocate in Illinois. Geisinger in Pennsylvania.
The regional nonprofit monopolies followed the same playbook: consolidate the market, capture the regulation, and make yourself unavoidable.
Dynasty 5: 340B Empires: The Safety-Net Exploiters
The 340B Drug Pricing Program was created in 1992 to help hospitals serving low-income patients stretch scarce resources.
It requires drug manufacturers to offer steep discounts to eligible “covered entities.” The hospital buys the drug cheaply, bills the insurer at full price, and keeps the spread.
A noble idea. But here’s what happened:
Hospitals realized they could expand their 340B eligibility by acquiring outpatient clinics — especially oncology practices, where drug costs are high. A single oncologist can generate $1 million in annual 340B profit for a hospital.
So they bought.
Between 2010 and 2021, hospitals dramatically increased their acquisitions of physician practices, particularly in specialties that use expensive drugs. 340B “child sites” exploded from 1,339 to over 36,000.
The patients served at these sites aren’t predominantly low-income. Studies show that 340B hospitals have been acquiring practices in wealthier neighborhoods with better payer mixes.
The program designed for the safety net became a spread trade for systems that don’t need it.
And the hospitals lobby furiously to keep it that way.
The Dynasty Advantages

$30 billion: AdvantageAnnual Value GME Funding (Academic Medical Centers)
$28 billion: Tax Exemptions (Nonprofit Hospitals)
$38+ billion: 340B Drug Program
34 states + D.C. with CON Protection
36,000+ (up from 1,339) with 340B Child Sites
Same denials. Same prior auths. Same moats. Different tax status.
The Inheritance
The Five Families: United, CVS, Elevance, Cigna, Centene, get the attention.
They’re publicly traded.
They answer to shareholders.
Their denials make the news.
But they didn’t build this system.
They inherited it.
Kaiser proved integration works. The academic medical centers captured GME funding, CON protection, and 340B eligibility. The Catholic systems consolidated under the mission. The regional monopolies showed that controlling beds means controlling the market. The safety-net exploiters turned a program for the poor into a profit center for the rich.
The Families looked at all of this and said, “We can do that too.”
The difference is that the Families are visible. The Dynasties kept their reputation.
What Now
This isn’t a broken system. It’s a rigged one.
The Dynasties wrote the rules. They captured the regulators. They built moats out of tax exemptions, CON laws, and federal funding streams that their competitors can’t access.
And they did it while calling themselves nonprofits.
The question isn’t whether you’re paying the tax. You are. Every premium, every facility fee, every surprise bill from a hospital outpatient department that used to be your doctor’s office.
The question is whether you understand why.
This Week: One Dynasty Per Day
Monday: Kaiser — The Integration Template
Tuesday: Academic Medical Centers — The Prestige Cartel
Wednesday: Catholic Systems — The Cross-Market Consolidators
Thursday: Regional Nonprofit Monopolies — The Payer-Provider Fortresses
Friday: 340B Empires — The Safety-Net Exploiters
The Dynasties have had it too easy for too long.
That ends this week.
If this satisfies something that needed to be said, become a paid subscriber.
Your support funds the journalism they don’t want published.
Dutch Rojas is a healthcare entrepreneur with multiple exits and the publisher of The Rojas Report. He is the author of Too Big To Care: How Nonprofit Health Systems Hijacked Healthcare.