
The Medicaid Subsidy Racket:
Where Equity Goes to Die

Let’s dispense with the bedtime story that Medicaid is the crown jewel of American health equity.
It isn’t.
It’s a bureaucratic protection racket—a Cold War-era compromise duct-taped into modern relevance wherein the rich in institutional power get richer, and everyone else is asked to perform moral gymnastics to survive.
Medicaid, in its current form, is less Florence Nightingale
and more Alan Greenspan meets Tony Soprano.
At the center of this policy farce is a two-tiered payment structure, which, if one squints hard enough, resembles a rigged casino masquerading as a public safety net.
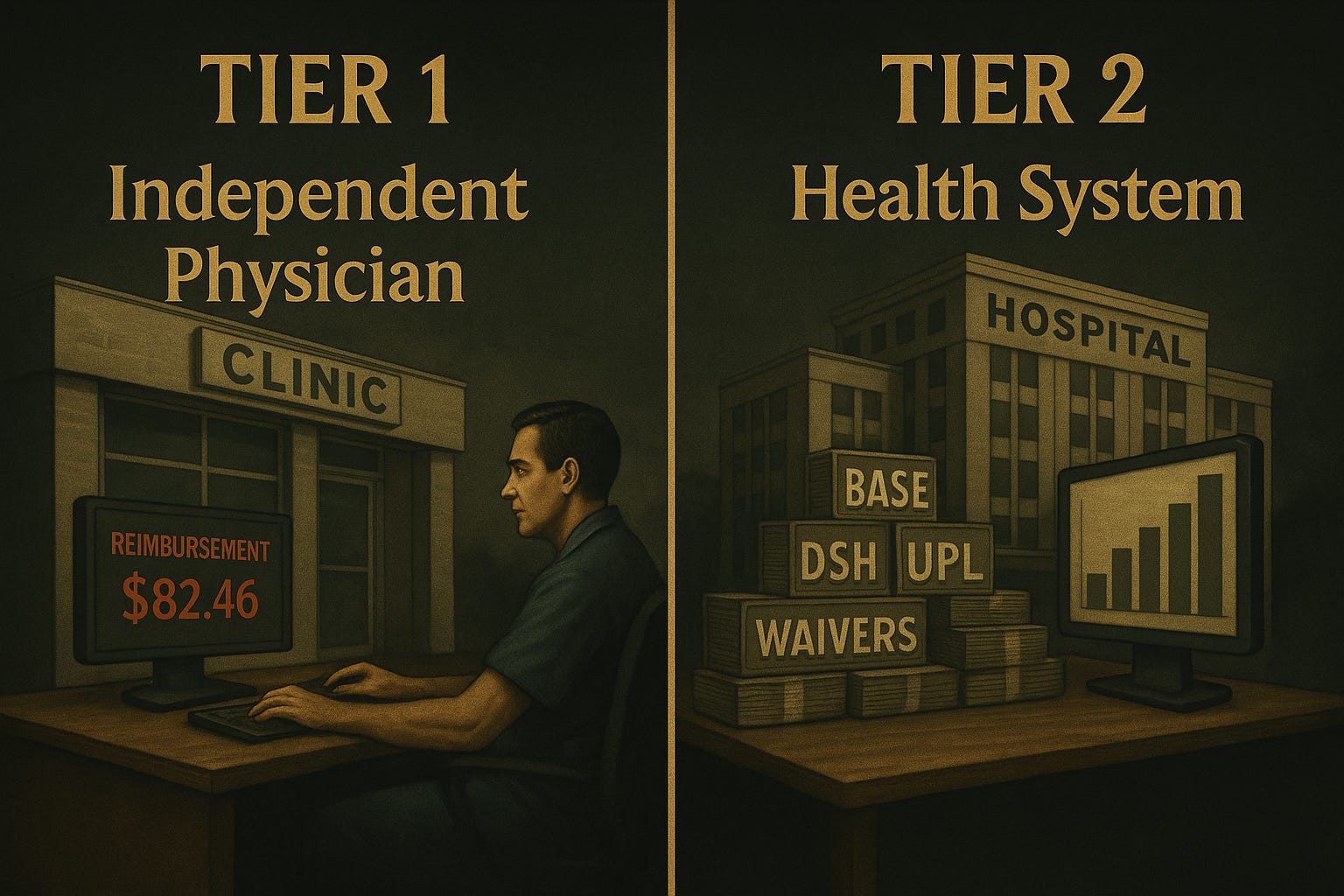
Tier One: The Great Pretend
Let’s begin with what’s publicly visible: Base Payments.
This is the fee schedule Medicaid offers to all physicians. In theory, it’s a standardized rate for standardized care. In reality, it’s an insult. The reimbursements are so low, they make Medicare look like a hedge fund bonus pool.
Here’s the recipe:
Add one part humiliatingly low rate
Stir in layers of administrative sludge
Bake under constant regulatory heat
Voila. You’ve got a system that punishes participation and labels it virtue.
Independent physicians who dare to engage with Medicaid find themselves in a Kafkaesque maze of billing codes, denials, and paperwork—all for the privilege of losing money per patient. Equity, we’re told, lives here. But it doesn’t. It lives somewhere else—behind the velvet rope.
Tier Two: The VIP Lounge of Public Funds
This is where things get interesting.
If base payments are the stale pretzels, supplemental payments are the caviar. However, this is only applicable to institutions with the proper credentials, relationships, and volume.
Welcome to Medicaid’s VIP room—a fiscal speakeasy accessed through back doors labeled:
DSH (Disproportionate Share Hospital)
UPL (Upper Payment Limit)
1115 Waivers
Intergovernmental Transfers
If none of those acronyms make sense, that’s by design. Medicaid’s true genius is not in delivering care, but in obfuscating the flow of money to those most politically connected.
Large health systems, many of which describe themselves as nonprofit, utilize these programs to conceal underpayments as financial windfalls. It’s not fraud, technically. It’s just… systematized favoritism.
An independent physician may bill Medicaid $50 for a consult and receive $42 (after clawbacks and denials). A health system bills the same, then leverages supplemental channels to walk away with $250—plus the moral applause of having “served the underserved.”
They treated the patient.
You got the bill.
They got the bonus.
Consequences (Intended and Otherwise)
Predictably, this two-tiered architecture doesn’t just distort incentives—it destroys markets.
Independent physicians exit Medicaid entirely.
Market consolidation accelerates, feeding the same institutional giants who benefit from subsidies.
Commercial payers absorb the cost shift, passing the burden to employers and working families.
Innovation stalls, because the only thing rewarded is scale, not results.
Medicaid, in effect, becomes a weapon. Not a safety net. Not a tool for inclusion. A gun is used to centralize control while performing equity theater for the cameras.

The Political Alchemy of Medicaid: From Safety Net to Stealth Public Option
The most astonishing trick of all? This transformation happened without a single national debate.
There were no fiery town halls. No public referenda. No breaking news banners.
Just a series of silent policy changes, administrative tweaks, and behind-the-scenes waiver approvals—ushering in a quasi-public option through Medicaid without ever calling it that.
Medicaid is now the largest insurer in the United States. Over 75 million people enrolled. Billions are flowing through managed care entities that get paid regardless of outcomes. And the public? Asleep at the wheel—convinced this is what compassion looks like.
But here’s the truth:
It’s not about poor patients.
It’s about political payments to influential players.

A Tempur-Pedic Throne of Lies
Suppose you still believe Medicaid is the great equalizer. In that case, you’re likely sitting on what Rory Sutherland might call a Tempur-Pedic throne of lies—comfortable, but built on cognitive dissonance and government incentives dressed as moral certainties.
The health systems know it. The states know it. The feds know it.
Only the independent physicians, who’ve been locked out of the bonus structure, are still asking, “Where’s our share?”
They won’t get it. Not without a fight.
The Path Forward
Here’s what we need:
Transparent funding flows. Show the public how the money moves.
Equity in supplemental payments. Stop treating “hospital” like a secret handshake.
Simplified Medicaid participation for independents. Remove the administrative chokehold.
Outcomes-based models. Pay for what works, not what scales.
Until then, Medicaid will remain what it is: a bureaucratic money printer for the powerful, and a bad punchline for everyone else.
The System Is Rigged. But It’s Not Unfixable.
This isn’t a conspiracy.
It’s policy by design, and it’s working precisely as intended.
But intention doesn’t equal virtue. And inertia is not destiny.
We can still turn the ship—if we stop moralizing and start disinfecting.
That begins with sunlight. Simplicity. And a little righteous anger.
The subsidy racket thrives in the dark.
Let’s flip the switch.
Are you in?
Or still defending the empire that buried the mission?
PHYCAPFUND.com
The system’s rigged—but the future doesn’t have to be.
PhyCapFund is closing its current round at the end of June, and we want you to join us.
We’re backing physician-led startups that are rewriting the rules of healthcare - no middlemen, no gimmicks, just results.
Want to see what we’re investing in next?
For a presentation on the hottest healthcare startups you’ve never heard of and for an opportunity to invest alongside your colleagues, send a message to info@phycap.com.