
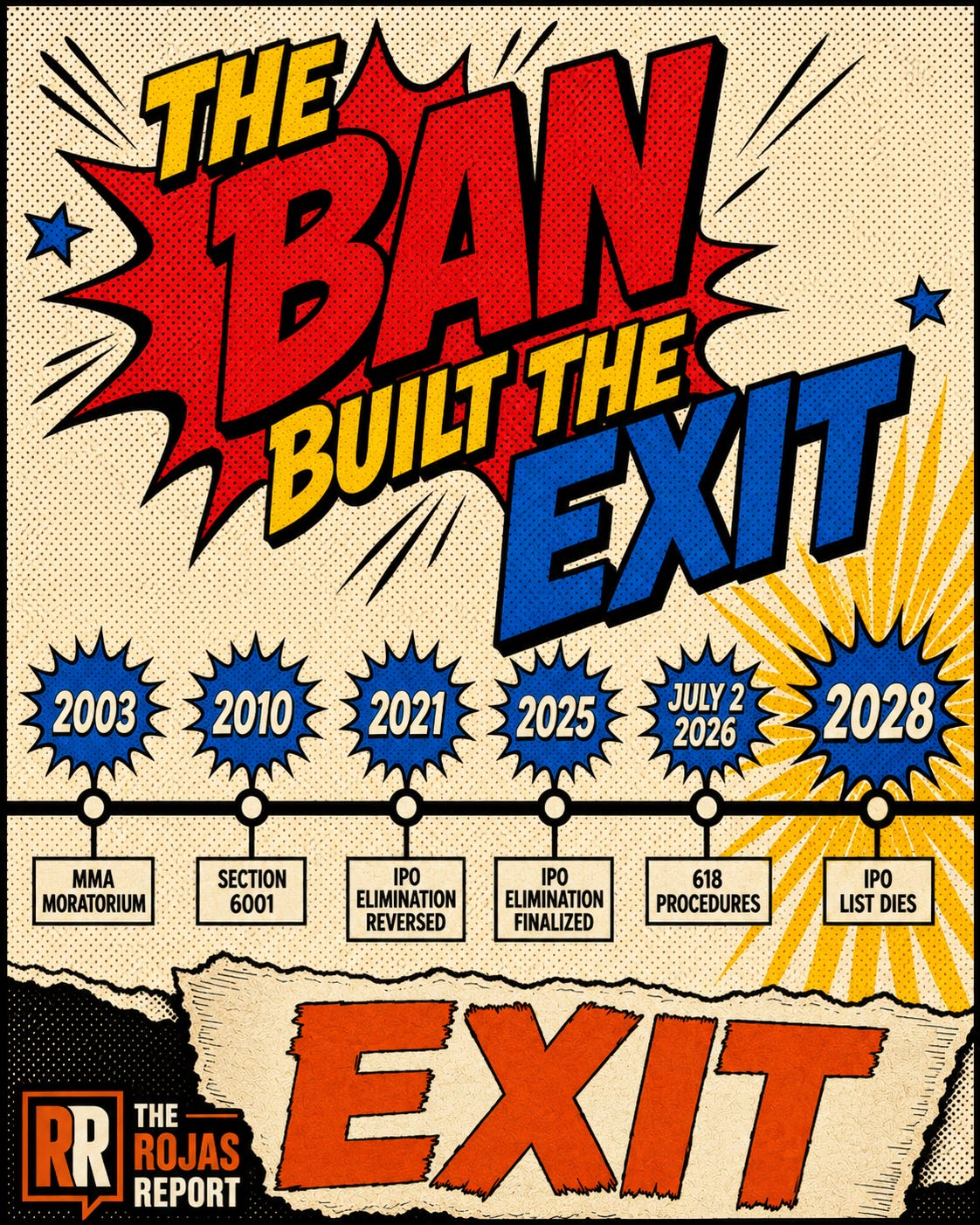
They Banned the Hospital. They Built the Surgery Center.
Section 6001 froze physician hospitals. It funneled physician capital into the one asset Washington never banned.

September 17, 2021. FAH sends CMS a letter.
CMS reverses its biggest outpatient policy in a decade.September 15, 2025.
FAH sends CMS the same arguments. Nearly word for word.CMS finalizes the policy anyway.
Four years.
Two letters.One reversal, one funeral.
What changed between those letters is worth more to independent physicians than anything Congress has passed in the past 20 years.
IN TODAY’S ARTICLE:
FAH opposed eliminating the In-Patient Only (IPO) list in 2021, and CMS reversed course. FAH ran the same arguments in September 2025, and CMS finalized the phase-out anyway. Both letters are public. The side-by-side is the story.
Section 6001 banned the creation of new physician-owned hospitals in 2010. ASC services were never designated health services under Stark, so the ban stopped at the surgery center door. Nobody ever even proposed extending it. Not FAH. Not the AHA. Not one think tank.
Sixteen years of containment followed: CON laws at the statehouse, site-neutral opposition in Washington, joint ventures everywhere else. Contain the price, contain the entry, buy the equity. Never touch the ownership.
FAH’s own members are hedged. Tenet’s USPI runs one of the largest ASC platforms in the country. The lobby defends the inpatient wall, while its members own the other side.
Glossary at the bottom of today’s article.
THE BEST DAY IN FAH HISTORY
March 23, 2010.
The Affordable Care Act becomes law. Buried in it sits Section 6001.
Section 6001 closed the Stark Law’s whole hospital exception. No new physician-owned hospitals. Grandfathered facilities frozen in place, barred from meaningful expansion.
For the Federation of American Hospitals, this was the summit of a campaign that ran the better part of a decade.
FAH lobbied for the inclusion of the 18-month moratorium on new physician-owned specialty hospitals in the Medicare Modernization Act in 2003.
It kept the pressure on through every subsequent rulemaking cycle. In 2010, it collected the permanent version.
The argument never changed.
Physician-owners cherry-pick the profitable, well-insured cases.
Community hospitals get the uninsured and the emergencies.
Ban the ownership, protect the community.
As a profession all physicians were found guilty.
Congress was cheap to buy.
The ban passed.
The lobby won.
Hold that thought, because the rest of this story is about what winning built.
THE BAN STOPPED AT THE SURGERY CENTER DOOR
The Stark Law prohibits physicians from referring Medicare patients to entities they own when those entities furnish designated health services.
Congress wrote that list in 1989 and expanded it in 1993.
Ambulatory Surgery Center services never made the list.
That is the entire legal architecture of the next sixteen years. Physician ownership of a hospital was covered by a named exception in an existing statute, so the lobby could run a closable loophole campaign. Physician ownership of an ASC was entirely outside the statute. Banning it required Congress to build a new prohibition from nothing.
Closing a loophole is a lobbying project.
Creating a prohibition is a war.
FAH chose not to fight it.
Here is the part that tells you everything: nobody else fought it either. Search the record. No FAH proposal. No AHA proposal. No think tank white paper. In the entire history of Washington health policy, no major organization ever formally proposed a federal moratorium on physician-owned ASCs.
Not because they liked the competition.
Because the weapon did not exist.
SIXTEEN YEARS OF CONTAINMENT
So the lobby fought with what it had.
Three levers. None of them touched ownership.
Price. Medicare pays hospital outpatient departments multiples of the ASC rate for identical procedures. Studies put physician-owned ASC cost savings above 50 percent against hospital settings. The lobby’s job was keeping that differential wide, and its weapon was the standby-capacity argument: hospitals need the markup to fund emergency readiness. Every site-neutral fight in Washington is an ASC suppression fight wearing a public safety costume.
Entry. More than half the states require a Certificate of Need to open or expand an ASC. Hospital associations built those laws and defend them session after session. The incumbents sit on the boards that judge the applications. They could not ban you in Washington, so they made you ask their permission in your state capital.
Equity. The Anti-Kickback Statute provides a safe harbor for hospital-physician joint-venture ASCs. When you cannot ban the competitor, buy into him. The health system takes the controlling position and the payer contracts. The physician performs the labor. The surplus rides the elevator upstairs.
Contain the price.
Contain the entry.
Own the equity.
For sixteen years, it worked.
Then CMS started moving the volume.
Every comment letter in this article is a public document.
The lobby’s business model assumes you will never read one.
100,000 physicians, healthcare executives, and lawmakers stopped cooperating:
Subscribe.
