
They Took Clinton’s Playbook. Then They Billed Your Patient.
In 1998, Bill Clinton parsed the word “is,” and the country laughed. The hospital lobby parsed five words in the 340B statute and built an $81 billion program on the definitions.

In 1998, President Bill Clinton parsed the word “is,” and the country laughed. The hospital lobby took notes.
Then hospital lobby parsed five words in the 340B statute and built an $81 billion program on the definitions.
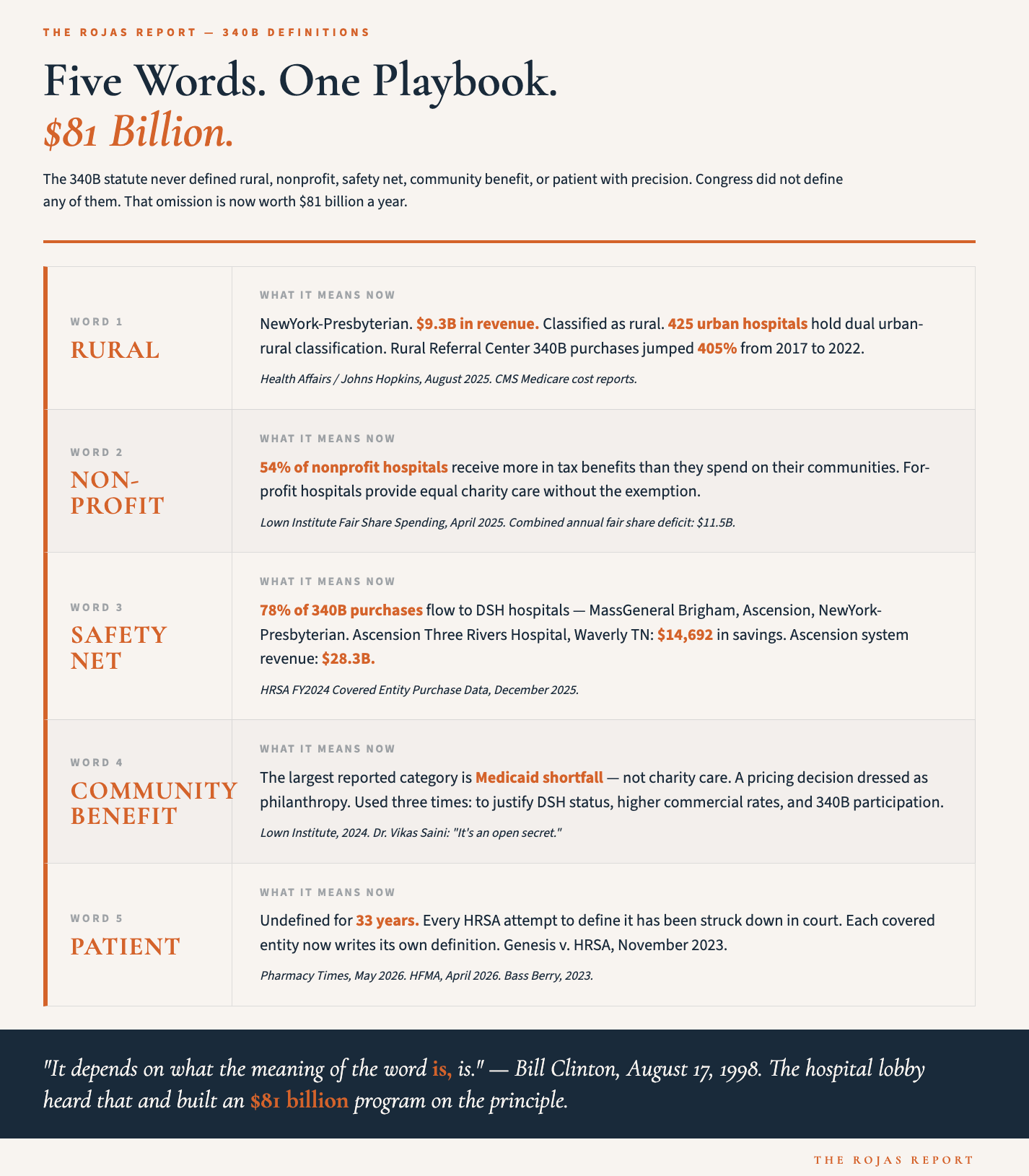
The words were rural, nonprofit, safety net, community benefit, and patient. None of them means what Congress intended anymore.
IN TODAY’S ARTICLE:
Five words in the 340B statute. What Congress meant when it wrote them. What they mean today.
“Rural”: how 425 urban hospitals became rural between 2017 and 2023 and what they captured in the process.
“Nonprofit” and “Community Benefit”: the Medicaid shortfall triple-dip that turns a pricing decision into philanthropy and collects three separate revenue streams from one line item.
“Safety Net”: 78% of 340B dollars flowing to DSH hospitals, the category that includes MassGeneral Brigham and Ascension.
“Patient”: 30 years, no workable definition. Every covered entity writes its own.
Glossary at the bottom of today’s article.
THE PLAYBOOK
Clinton’s answer was mocked as the most lawyerly evasion in American political history. Parse a single word. Change the meaning. Escape the consequence.
The hospital lobby watched that and thought: We can do this at scale.
Congress passed the 340B Drug Pricing Program in 1992. The statute runs 800 words. It contains five terms that carry the entire weight of the program’s eligibility architecture. Rural. Nonprofit. Safety net. Community benefit. Patient.
Congress did not define any of them with precision.
That omission is now worth $81 billion a year.
In the thirty years since 1992, the hospital industry has systematically lobbied, litigated, and regulated each of those five words into something Congress never intended. Not by breaking the law. By rewriting what the words mean. One definition at a time. One regulatory filing at a time. One court ruling at a time.
Clinton was defending himself. The hospital lobby was enriching itself. Same mechanism. Different stakes.
The patient pays the bill.
RURAL
Congress wrote the lower 340B eligibility threshold for rural referral centers to help large regional hospitals that genuinely served rural patient populations.
Three hospitals held dual urban-rural classification under Medicare in 2017.
By 2023, 425 hospitals held it.
Yang Wang at the Johns Hopkins Bloomberg School of Public Health led the research. Health Affairs published it in August 2025. The data came from official CMS Medicare cost reports and impact files covering 2013 through 2023.
Here is what the data found at the top of the list.
NewYork-Presbyterian Hospital. 2,850 beds.
Nearly $9.3 billion in net patient revenue.
Classified as rural for Medicare purposes.
Cleveland Clinic.
$7 billion in revenue.
Classified as rural.
UCSF Medical Center, San Francisco.
$6.1 billion in revenue.
Classified as rural.
AdventHealth Orlando.
$6.2 billion in revenue.
Classified as rural.
Cedars-Sinai Medical Center, Los Angeles.
$4.3 billion in revenue.
Classified as rural.
The mechanism was a 2016 CMS rule change following two federal appellate court rulings. Urban hospitals could now carry both urban and rural classifications simultaneously. Urban wage index for Medicare payment. Rural eligibility for 340B. The same address. Two definitions. Zero tradeoff.
Rural Referral Center 340B purchases jumped 405% from 2017 to 2022, reaching $1.3 billion. That is more than the combined 340B purchases of critical access hospitals and sole community hospitals combined. The two categories for which Congress actually wrote the rural framework.
Congress wrote the word rural for Madelia, Minnesota. NewYork-Presbyterian collected it in Manhattan.
The AHA formally registered H.R. 7409, the Defend Rural Health Act of 2026, as a lobbying target in its Q1 2026 federal disclosure, filed April 20, 2026.
That same filing lists “rural reclassification policy” as an active lobbying concern. The bill to close the loophole is sitting in Congress. The AHA’s lobbyists are registered on it.
That is what the word rural means in 2026.
The hospital lobby spent 30 years rewriting the definitions.
This is where the receipts live.
Become a paid subscriber. $49.99 a month. $300 a year. Subscribe
