
They Trained Your Doctor. Then They Rigged the Game.
Six moats. $30 billion in annual subsidies. The architects of American healthcare’s pricing crisis.

Yesterday, I showed you Kaiser, the integration template.
The nonprofit that proved the model and the denials.
Today, the institutions that trained every doctor you’ve ever seen.
And captured every regulatory advantage while doing it.
The Prestige Shield
Hopkins. Penn. Duke. Cleveland Clinic. Mayo. UPMC. Mass General Brigham. NYP. Yale-New Haven. Vanderbilt.
These are sacred names in American healthcare.
They train the doctors.
They conduct the research.
They treat the most complex patients.
They publish the studies everyone cites.
This is real. But it’s also a shield.
Because while you were admiring the prestige,
they were capturing every regulatory advantage in American healthcare.
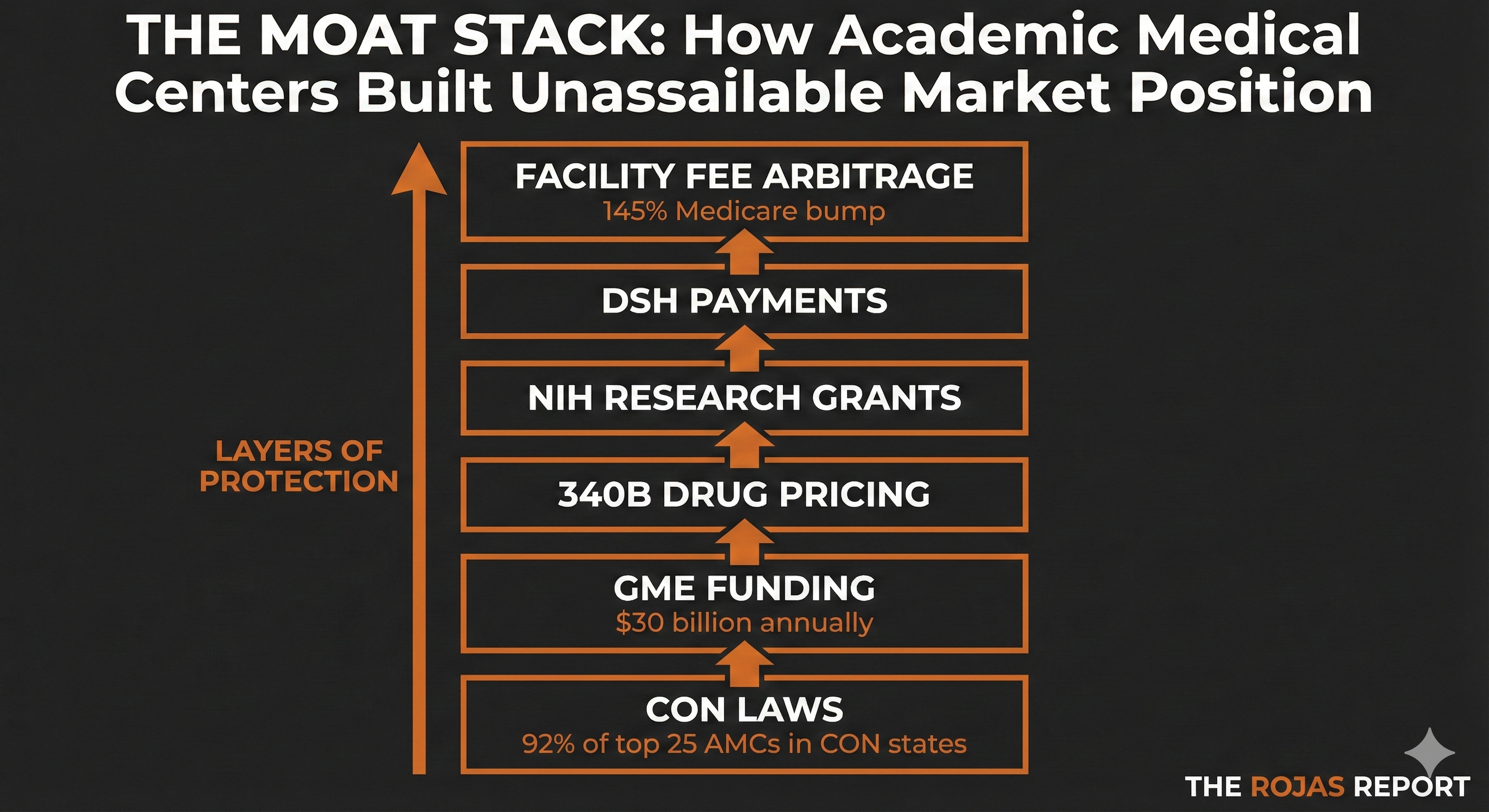
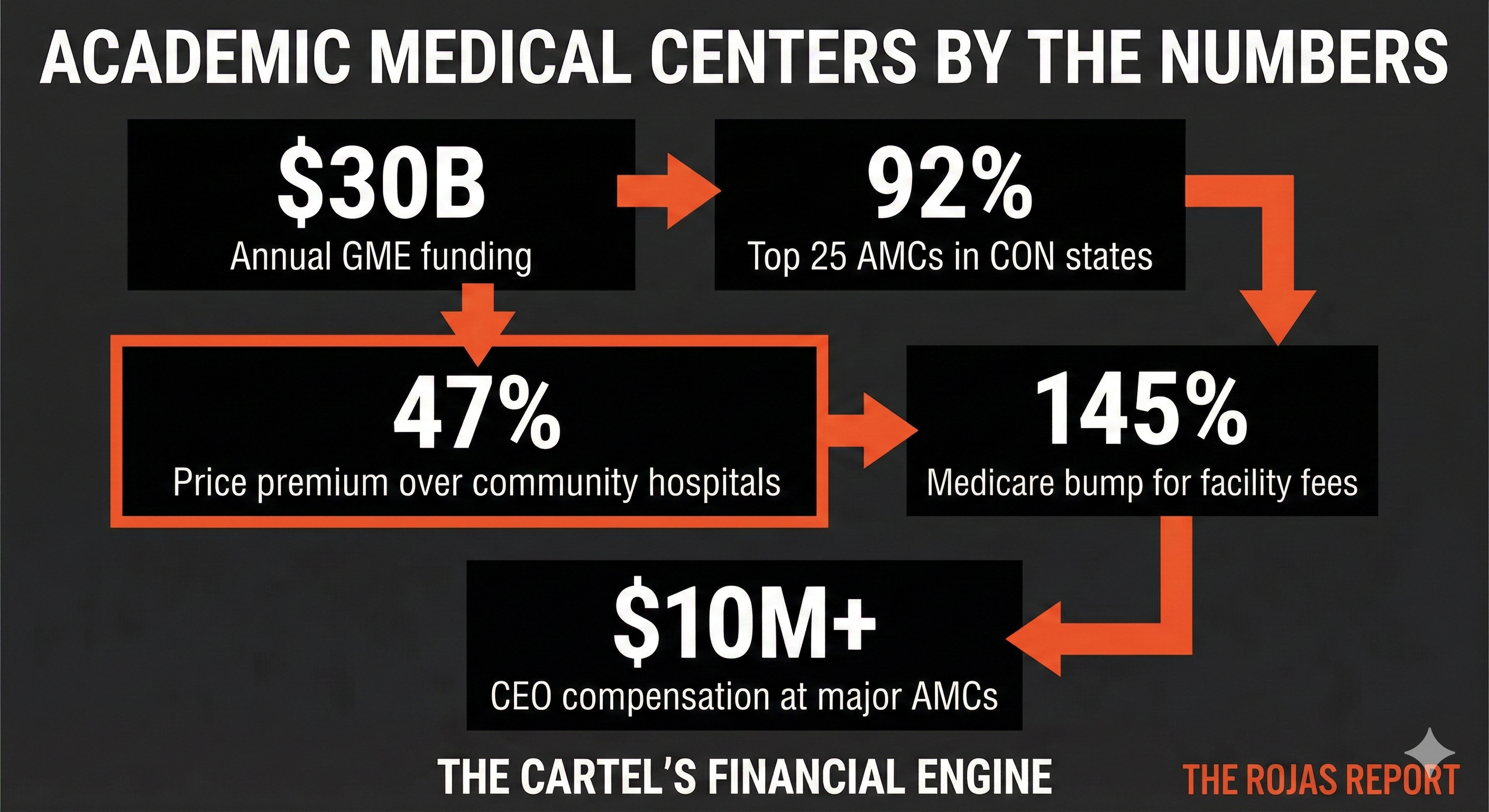
$30 billion in annual Graduate Medical Education payments.
92% of the top 25 academic medical centers operate in Certificate of Need states.
47% higher prices than community hospitals, for the exact same procedures.
They didn’t just build great institutions.
They built fortresses.
The Moats
Let me show you how the game works.
Moat #1: Graduate Medical Education, $30 Billion a Year
Every residency program in America runs through hospitals. Most of those dollars flow to academic medical centers.
$30 billion annually from Medicare to fund physician training.
The AMCs control residency slots. They decide how many doctors get trained, in which specialties, and in which cities.
This isn’t just money. It’s a labor pipeline.
When you train residents, you get subsidized labor for 3-7 years. Residents work 60-80-hour workweeks at a fraction of attending physician salaries. The GME payment is supposed to cover their training. In practice, it subsidizes the hospital’s labor force.
And when those residents finish? Many stay. The AMC that trained them often employs them.
The academic medical centers didn’t just capture training funding. They captured the profession.
Moat #2: Certificate of Need. The Competitor Veto
In 35 states plus DC, you need government permission to build a hospital, add beds, or buy major equipment.
Who decides? Boards are often influenced by incumbent hospitals.
92% of the top 25 academic medical centers operate in certificate of need (CON) states.
That’s not a coincidence. That’s strategy.
CON laws let AMCs veto their competition. When an ambulatory surgery center tries to open, the AMC can file an objection. When a physician group wants to build an imaging center, the AMC can slow-walk it through regulatory hell.
The University of Iowa — the state’s academic medical center — was denied the right to build a new hospital because competitors argued it would hurt their business.
The competitors got a vote.
That’s CON.
Moat #3: 340B Drug Pricing. The Spread Trade
The 340B program forces drug manufacturers to sell at steep discounts to hospitals serving low-income patients.
AMCs qualify. Many have Disproportionate Share Hospital status.
Here’s the arbitrage: Buy drugs at 340B prices. Bill insurers at full price. Keep the spread.
One oncologist can generate $1 million in annual 340B profit — for the hospital, not the patient.
The AMCs have been on an acquisition spree for oncology practices. Now you know why.
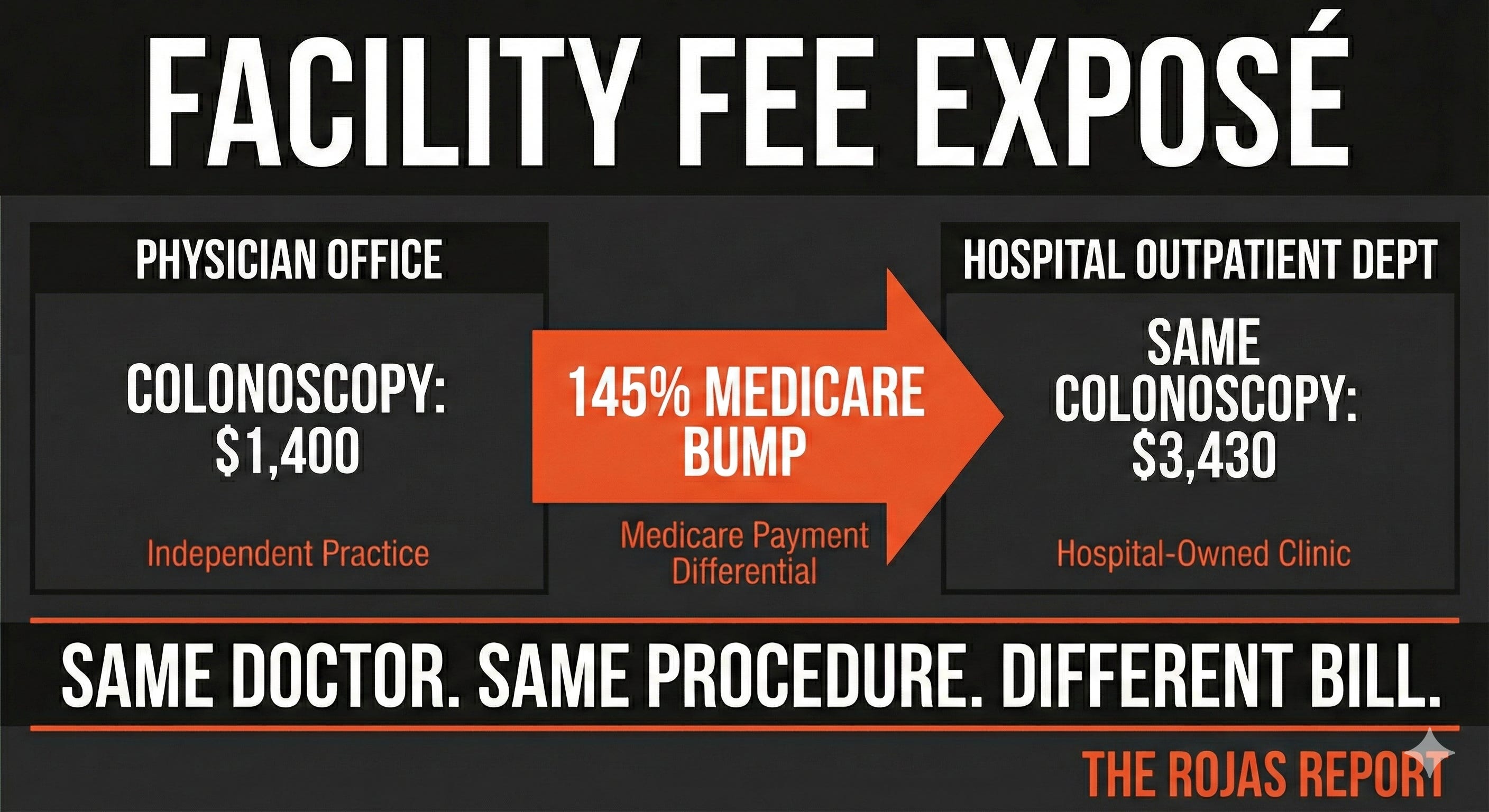
Moat #4: The Facility Fee Goldmine
This is the most elegant extraction mechanism in healthcare.
When an AMC acquires a physician practice and converts it to a “Hospital Outpatient Department,” Medicare pays 145% more for the exact same service.
Same doctor. Same exam room. Same stethoscope.
Different bill.
A colonoscopy in a physician’s office: ~$1,400.
The same colonoscopy in a hospital outpatient department: ~$3,430.
Nothing changed except the sign on the door and who deposits the check.
This is why AMCs have been buying physician practices for two decades.
Every independent practice they acquire becomes a facility fee revenue generator.
The American Hospital Association fights site-neutral payment reform harder than almost any other policy issue.
Now you know why.
The Health Plan Problem
Here’s what most people don’t realize:
Academic medical centers own health plans.
Hopkins has one. Mass General Brigham owns a Medicaid plan. UPMC Health Plan is the largest insurer in Western Pennsylvania.
When an AMC owns the insurance and the hospital, it controls both the premium and the denial.
The academic prestige doesn’t stop them from building the same utilization management infrastructure as Aetna.
Same prior authorizations. Same claim denials. Same appeals processes.
They just do it with nicer lobbies and better PR.
The Outcome Paradox
Here’s the uncomfortable truth:
For most conditions, AMCs don’t deliver better outcomes than good community hospitals.
They excel at the most complex cases. Rare cancers. Transplants. Experimental procedures. The cases that require the full weight of a research institution.
But for bread-and-butter healthcare, joint replacements, routine surgeries, chronic disease management, community hospitals and physician-owned facilities often match or beat AMC outcomes.
At a fraction of the price.
The prestige justifies the pricing.
The data often doesn’t.
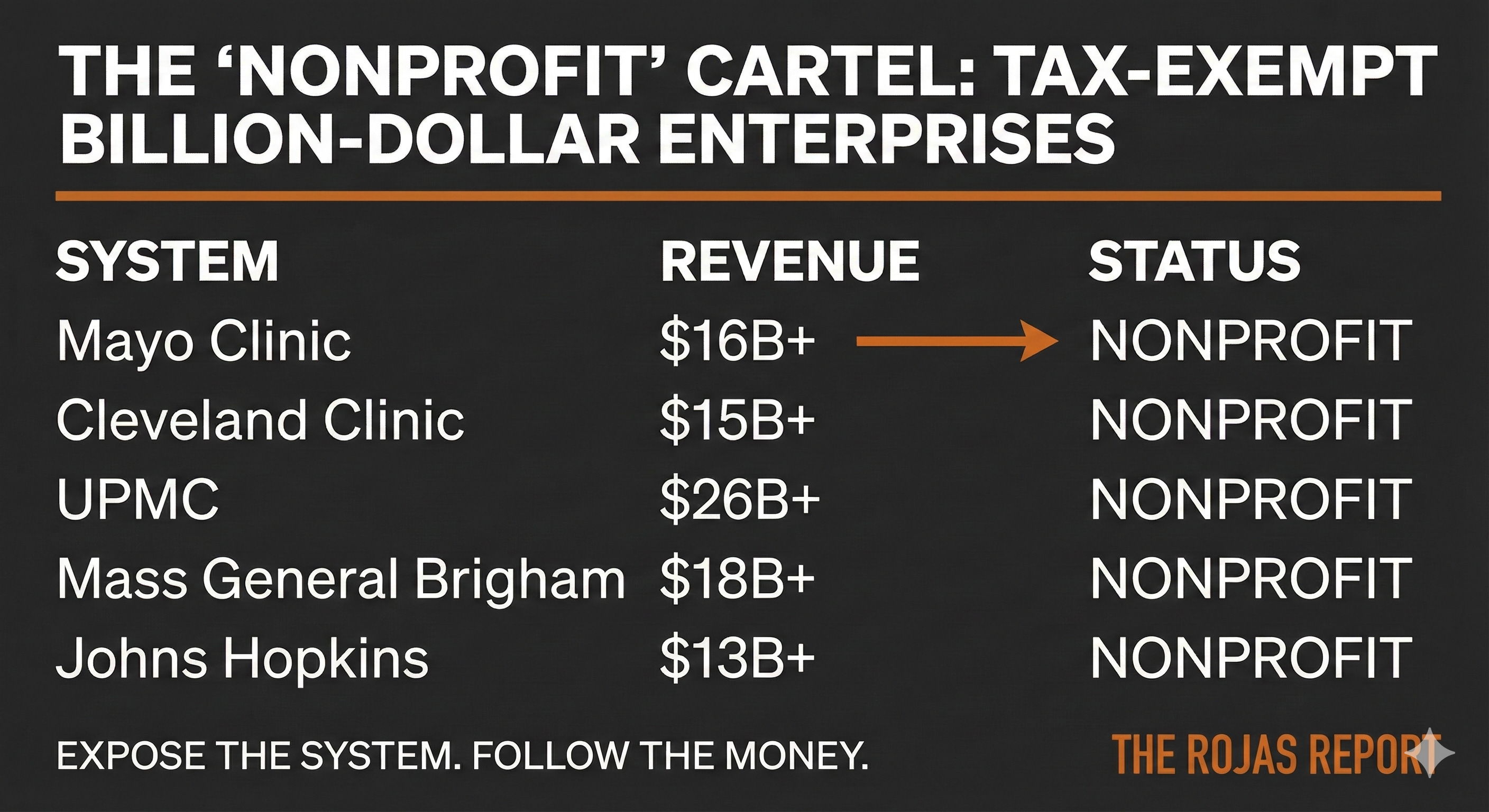
The Names
Let me name them.
Cleveland Clinic
$15+ billion in revenue. Nonprofit status. Massive commercial real estate holdings. Aggressive physician practice acquisition across Ohio, Florida, and now London and Abu Dhabi.
Mayo Clinic
$16+ billion in revenue. A destination medicine model that serves wealthy out-of-state patients while claiming Minnesota nonprofit tax benefits. Is it a surprise that Minnesota has had a moratorium on hospitals since 1987?
UPMC
Controls approximately 70% of the Pittsburgh hospital market. Operates one of the state’s largest health insurers. CEO compensation exceeding $10 million. Nonprofit.
Johns Hopkins
Historic prestige. Billions in NIH funding. Aggressive expansion throughout Maryland and into other states. One of the most recognized brands in medicine.
Mass General Brigham
Dominates the Boston market. Premium pricing justified by the Harvard name. Expanding footprint across New England.
Duke Health
Dominates North Carolina alongside UNC. Benefits from one of the nation’s oldest and most restrictive CON laws.
NewYork-Presbyterian
Columbia and Cornell. Two Ivy League brands. Manhattan pricing.
Penn Medicine
Philadelphia’s dominant system. The University of Pennsylvania brand is commanding premium rates. Aggressive regional expansion.
These are not struggling charities.
These are billion-dollar enterprises with monopoly power, operating under nonprofit protection.
The Real Architects
Here’s what I want you to understand:
The MBAs at UnitedHealth didn’t invent vertical integration.
They didn’t dream up facility fee arbitrage.
They didn’t figure out how to capture regulatory moats.
The academics did.
The physician-administrators at Hopkins, Penn, and UPMC figured out decades ago how to build moats out of regulations and call it community benefit.
The Five Families watched.
They took notes.
They ran the spreadsheets.
Then they scaled what the academics had already built.
The students became the villains.
The teachers kept their reputation.
The Lobbying Machine
AMCs are disproportionately powerful in healthcare lobbying.
They have prestige. When a Cleveland Clinic executive testifies before Congress, they’re treated as an authority, not an interested party.
They have alumni networks that include senators, governors, and cabinet members.
They have research relationships with NIH and FDA that create institutional dependencies.
When an AMC president calls a congressional office, the call gets taken.
When an independent physician calls, they get voicemail.
This influence shapes policy:
→ GME funding flows to AMCs, not community hospitals
→ Research funding prioritizes academic centers
→ CON laws protect established players
→ The physician-owned hospital ban eliminates competition
→ Site-neutral payment reform dies in committee
The academic mission provides cover.
The lobbying protects the business model.
Tomorrow: Dynasty 3
Tomorrow we move to the Catholic Systems, CommonSpirit, Ascension, Providence, Trinity.
Ministry on the letterhead.
Private equity math in the boardroom.
Five of the ten worst “fair share deficits” in American healthcare.
$28 million CEO compensation at CommonSpirit.
The Cross-Market Consolidators.
For Paid Subscribers: Saturday
The Physician Playbook: Competing Against Academic Medical Centers
If you’re an independent physician competing against an AMC, you’re not just competing against a hospital. You’re competing against a fortress with six different moats, a century of prestige, and a lobbying operation that reaches into every committee room in Washington.
Saturday’s paid-only piece breaks down:
Where the AMC model is vulnerable
How independent practices can compete on quality and service?
The employers who are tired of paying the prestige premium
What site-neutral payment reform would actually mean
The Five Dynasties Series
Today: Academic Medical Centers.
The Prestige Cartel ← You are here
Tomorrow: Regional Monopolies. The Payer-Provider Fortresses
Friday: 340B Empires. The Safety-Net Exploiters
If this satisfies something that needed to be said, become a paid subscriber and give the gift of knowledge to fellow physicians and healthcare advocates. Your support funds the journalism they don’t want published.
Subscribe to The Rojas Report
Give the Gift of The Rojas Report
Dutch Rojas is a healthcare entrepreneur and the publisher of The Rojas Report. He is the author of Too Big To Care: How Nonprofit Health Systems Hijacked Healthcare.
Rojas out.
