
University Hospitals Built the One Business That Cannot Lose. They Made You the Backstop.
The academic medical center keeps every dollar of margin in the good years and hands the losses to the legislature in the bad ones. That is not a charity. That is a backstopped monopoly.

A business that keeps all the profit and absorbs none of the loss does not exist.
Except it does.
It runs your region’s largest hospital.
And it trained your doctor.
IN TODAY’S ARTICLE:
How the university hospital captures every margin and offloads every loss onto the state
The four extraction mechanisms: practice acquisition, facility fees, must-have pricing, and the 340B spread
Why the state cannot let the system fail once it owns the region, and what that does to your tax bill
Where this series goes next: the individual systems, one at a time, by name
Glossary at the bottom of today’s article.
THE BUSINESS THAT CANNOT LOSE
They told you the academic medical center serves three missions.
Care.
Education.
Research.
A public-spirited institution, too important to question.
Look at the balance sheet instead.
The modern university health system is a multi-billion-dollar conglomerate that solved the one problem every other business spends its life fighting. Risk. It captures the upside of a commercial monopoly and carries the downside of a public utility. When the margins come in, the system keeps them. When the losses come in, the state covers them.
Heads it wins.
Tails you pay.
That asymmetry is not an accident of the model. It is the model.
HOW THEY CAPTURE THE UPSIDE
The machine runs on four mechanisms.
Each one is legal. Together they are extraction.
One. They buy the competition.
The share of physicians employed by hospitals climbed from roughly 25% in 2012 to over 85% by 2024. University systems led the charge. UPMC alone controls more than 60% of hospital beds in Allegheny County and employs over 70% of the region’s physicians. The independent physician faces one choice. Sell the practice to the system, or get cut out of the referral networks and insurer panels the system already owns.
Avalere put a number on what survives. Across cardiology, gastroenterology, medical oncology, orthopedics, and urology, just 12% of practice remains unaffiliated and independent.
Two.
They reprice the same care.
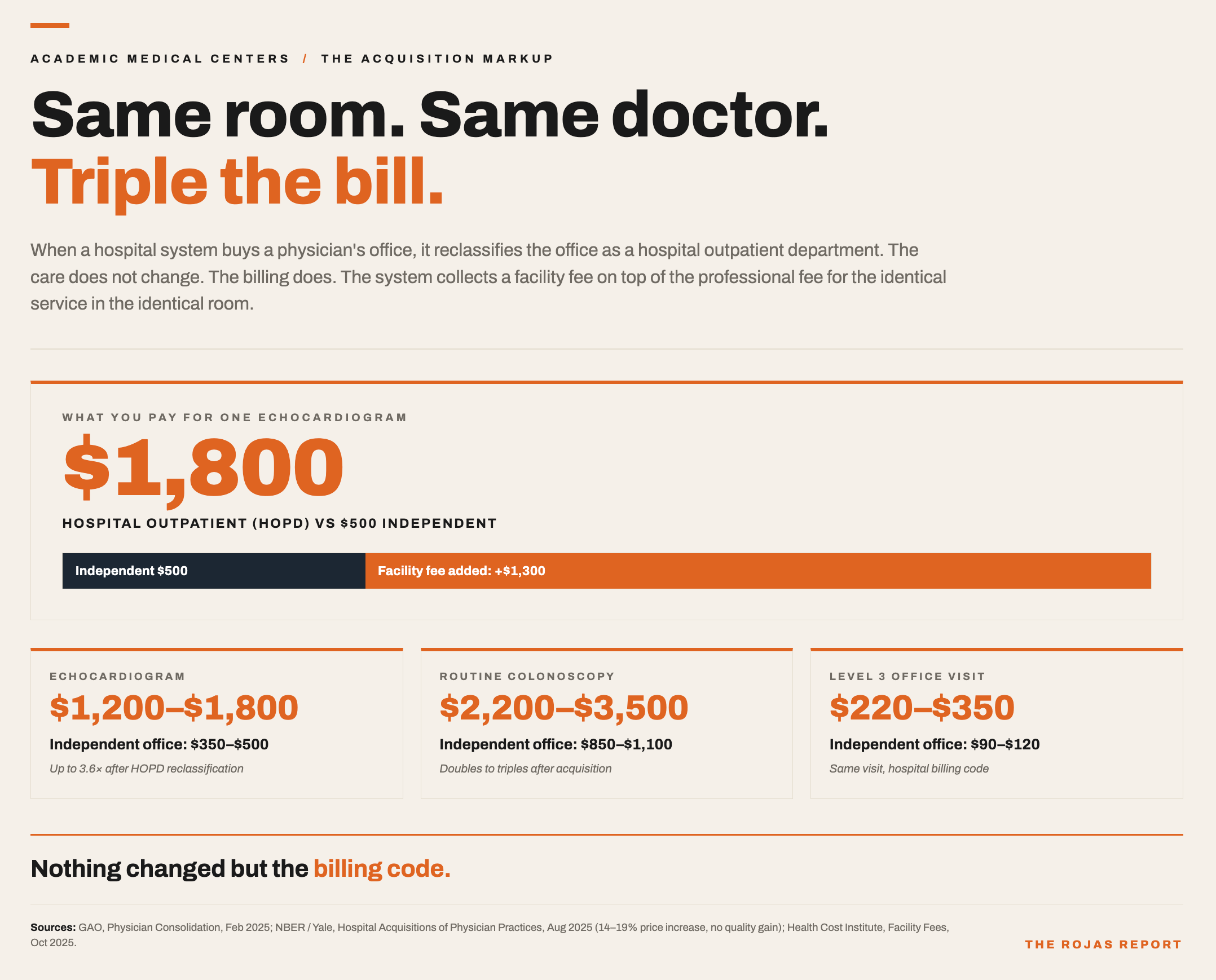
When the system acquires your cardiologist’s office, it reclassifies that office. Nothing about the care changes. The billing does. Now the system collects a facility fee on top of the professional fee for the same service in the same room.
The NBER measured it. Hospital takeovers of physician practices drove prices up 14% to 19%, with no measurable improvement in outcomes. An echocardiogram that costs $350 to $500 in an independent office costs $1,200 to $1,800 after the facility fee. A routine colonoscopy doubles or triples.
Three. They become unavoidable, then price like it.
Once a system owns the region, no insurer can sell a plan without it. That is leverage, and the prestige brands use it. The RAND Hospital Pricing Study, Round 5, found prominent academic medical centers collecting between 250% and 450% of Medicare rates for the same services.
Sutter Health showed what enforcing that leverage looks like. All-or-nothing contracting. Anti-steering clauses. Sutter paid $575 million to California and its employers in 2021, then another $228.5 million in 2025 on the eve of a federal retrial. The playbook was the point.
Four. They run the drug spread.
Congress built the 340B program in 1992 so safety-net hospitals could buy outpatient drugs at deep discounts and stretch scarce resources. The statute never capped what the hospital could collect from a commercial insurer for those same drugs. So the academic systems buy at a 25% to 50% discount, collect the full commercial price, and keep the difference.
Duke booked $282 million in 340B profit over five years. The program swelled into an $81 billion market by 2024. In April 2025, the HELP Committee report named Cleveland Clinic and Bon Secours Mercy Health for generating hundreds of millions in 340B revenue while passing no direct discounts to patients. Conti and Bach documented the tell years earlier. The new 340B clinics open in wealthier, better-insured ZIP codes, not the poor neighborhoods the program was written for.
You cannot buy a kind word in The Rojas Report.
That is exactly why more than 100,000 readers believe it.
Thank you to our supporters!
Subscribe to continue.
Keep reading with a 7-day free trial
Subscribe to The Rojas Report to keep reading this post and get 7 days of free access to the full post archives.