
The University of Missouri Health Is Not a Hospital. It Is the State of Missouri.
Section 115 of the IRS turns a $1.9 billion hospital empire into an entity that is structurally incapable of paying taxes. And now it wants the legislature to give it 25 more counties.

A nonprofit hospital is tax-exempt.
You knew that.A state hospital is something different.
It is the state.University of Missouri Health Care does not file a Form 990.
There is nothing to file. The state does not pay taxes to itself.And now it wants legal permission to acquire 25 counties of rural hospitals without antitrust review.
Essential Context: The State of Missouri is represented by two of the most influential lawmakers in the naiton. Congressman Jason Smith, Chairman of Ways and Means substantial and Senator Josh Hawley who sits on Senate HELP. Both of these committee assignments have direct oversight on American Healthcare policy.
IN TODAY’S ARTICLE:
Why Section 115 of the Internal Revenue Code makes The University of Missour Health a different kind of tax-exempt than the one you are thinking of
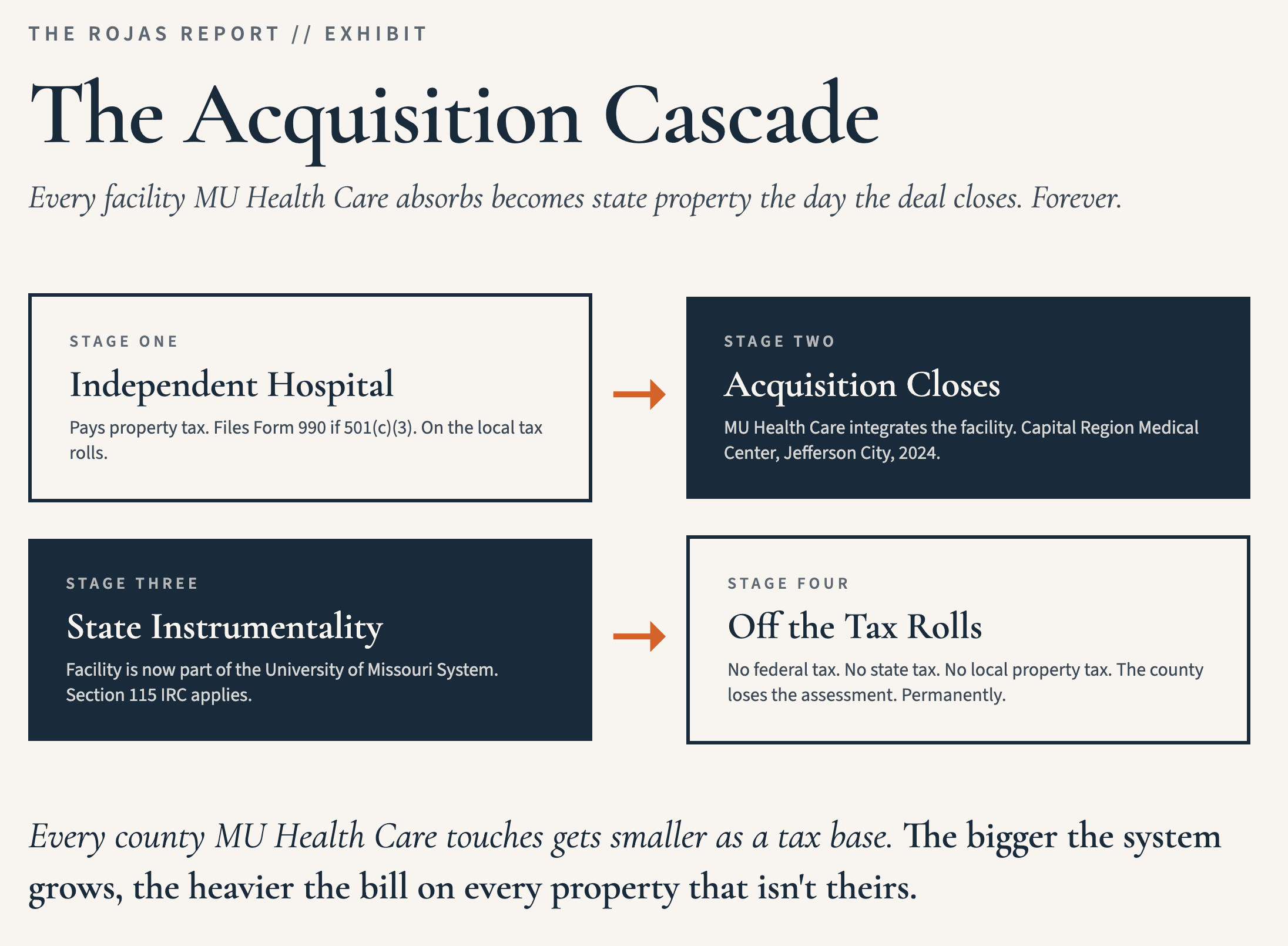
With every acquisition the system makes, it converts taxable property into state property, permanently.
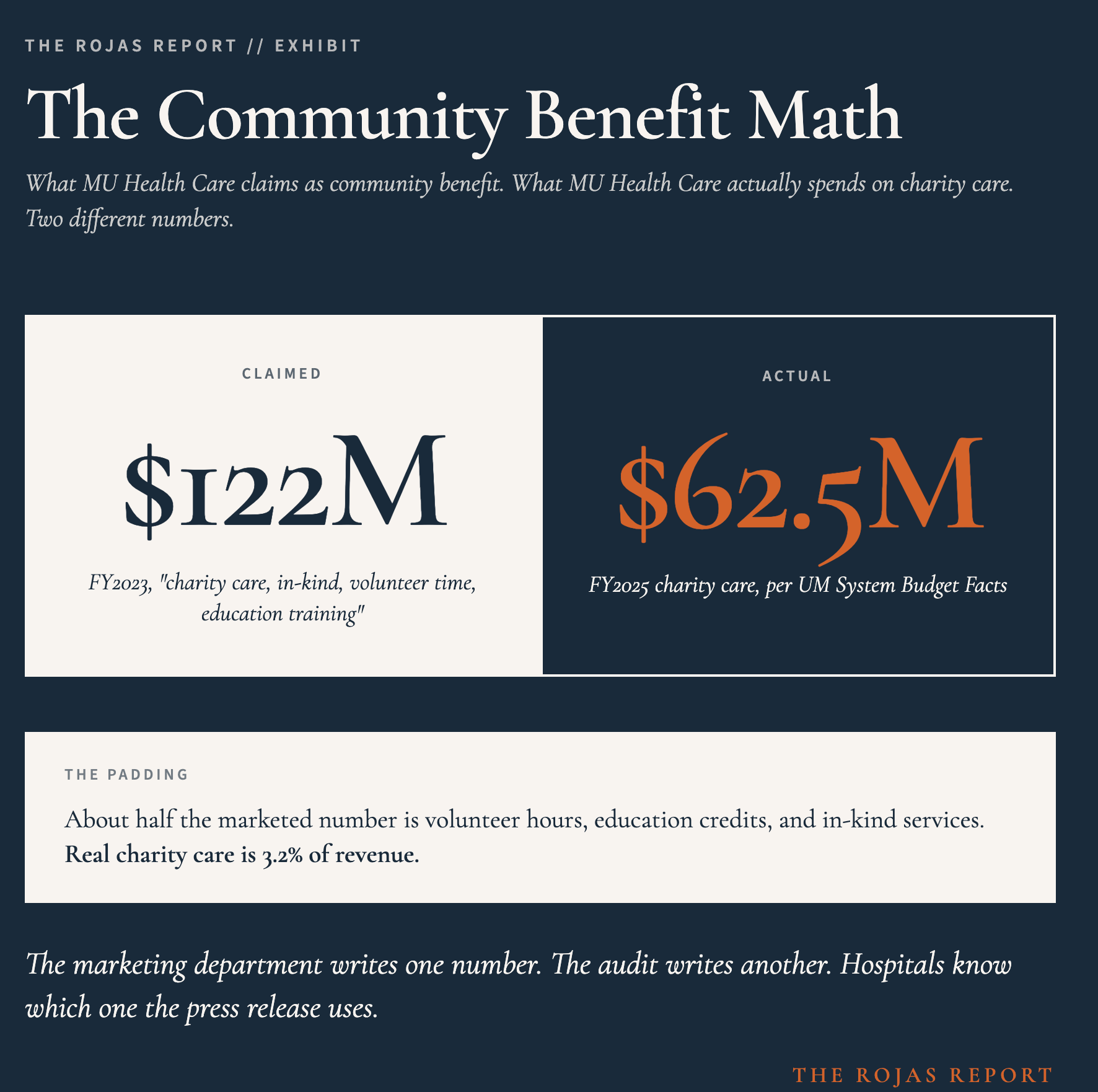
The math of $122 million in claimed “community benefit” against $62.5 million in actual charity care
Why the antitrust immunity bill is the closing argument, not the opening
Glossary at the bottom of today’s article.
THE STATE DOES NOT PAY TAXES TO ITSELF
Most readers know what a 501(c)(3) hospital is. A nonprofit. A tax-exempt corporation organized under federal law. Files a Form 990 every year. Has to publish executive compensation. Has to claim community benefit to keep the exemption.
University of Missouri Health is none of those things.
It is not a 501(c)(3). It does not file a Form 990. It does not have to defend its exemption every year because there is no exemption to defend. The University of Missouri Health is a state instrument, organized as part of the University of Missouri System, governed under Section 115 of the Internal Revenue Code.
Section 115 excludes income derived by a state from the exercise of essential governmental functions from gross income. The state does not pay federal income tax to itself.
That is the starting position.
Every other tax exemption flows from there. No federal income tax. No Missouri state income tax. Zero property tax on the entire portfolio: the 390-bed flagship University Hospital, the Women’s and Children’s Hospital, Ellis Fischel Cancer Center, Missouri Orthopaedic Institute, Missouri Psychiatric Center, and dozens of clinics across mid-Missouri.
Boone County collects nothing from any of it.

THE TAX CANNIBAL
Here is one reason you read The Rojas Report.
Every facility the University of Missour Health acquires becomes part of the state. On the day the deal closes, that facility ceases to be a taxable asset.
Forever.
In 2024, the system fully integrated Capital Region Medical Center in Jefferson City. Capital Region was a separate nonprofit before the integration. Now it is state property. Cole County and the City of Jefferson City no longer assess it the same way.
This is not a one-time event. Capital Region was the largest of a sequence. The University of Missouri Health has opened owned clinics and urgent care locations in Audrain County and in Mexico, Missouri. Each one of those is state property the day it opens. None of them generates property tax for the counties they sit in.
The pattern is the cannibal. Every time The University of Missiouri Health grows, the local tax base shrinks.
Every hospital The University of Missouri swallows leaves the tax rolls forever. 60,000+ physicians and healthcare operators track acquisitions on this newsletter because the announcement comes after the deal is closed. By then, the rolls have already shifted.
THE NUMBERS THE STATE DOES NOT PUBLISH
Now look at the scale of what is already inside the moat.
In Fiscal Year 2025, The University of Missouri Health reported $1.91 billion in total operating revenue. That is up from $1.77 billion in FY2024 and $1.41 billion in FY2023. The University of Missouri System has budgeted $2.12 billion in net revenues for FY2026. Every dollar of that flows through an entity that does not pay federal income tax, does not pay Missouri income tax, and does not pay property tax.
Total assets at the end of FY2025: $1.97 billion. Total net position: $1.22 billion. Operating income for the year: $68.4 million. Net position grew by $107 million over the past 12 months.
A university health system with $1.22 billion in net worth that adds $107 million a year is not a struggling safety net. It is a corporation. The phrase “safety net hospital” is a tax classification, not a financial diagnosis.
$918,465
The CEO of the University of Missiour Health is Ric Ransom. He took the job in May 2023, replacing interim CEO Nim Chinniah, who replaced Jonathan Curtright. Ransom holds a JD, an MBA, and an MSHA. He came from the University of Wisconsin Hospitals system and, before that, ran operations at Greenville Memorial Hospital in South Carolina.
In 2024, his annual salary was $918,465.
That figure is on the public payroll. Ransom is a state employee. There is nothing hidden about it. It is just not reported.
In FY2025, total compensation and benefits across the entire system reached $789 million. The system spent $62.5 million on charity care that year. The compensation line is roughly 12.6 times the charity line.
This is not corruption. There is no scandal. The state is paying market rate for an academic medical center CEO. The point is what the structure produces. A state instrumentality, exempt from every meaningful tax, that pays Wall Street wages while writing off 3.2% of revenue to the poor.
A state employee earning $918,465 is not a secret. It is just not reported. The Rojas Report names the salaries that other publications round down.
THE COMMUNITY BENEFIT MATH
Hospital community benefit is the line item that justifies tax exemption. It is supposed to mean charity care. In practice, it almost never does.
The University of Health publishes a page called “Our 340B Story.” On that page, the system claims $122 million in “charity care, in-kind health services, volunteer time, and health education training” for FY2023.
Read that sentence again.
Charity care, in-kind, volunteer time, and education training.
Those are four different things in one number.
The University of Missouri System’s own Budget Facts FY2026 reports actual charity care for FY2025 at $62.5 million. Even adjusting for the year difference, the implication is clear. About half of what the system markets as community benefit consists of volunteer hours, education credits, and in-kind padding that cost the system little to nothing.
The $62.5 million in actual charity care is 3.2% of FY2025 revenue.
The padded $122 million figure makes it look like 6.4%.
That is the entire community benefit industry. Not just here. Everywhere. The Lown Institute audits hospital fair-share spending nationwide and finds the same gap at most tax-exempt systems.
340B AS PROFIT CENTER
The 340B Drug Pricing Program is supposed to help safety-net hospitals stretch federal resources. Hospitals get steeply discounted drug pricing, then dispense those drugs to insured patients at full reimbursement. The spread is the savings.
In FY2023, The University of Missouri Health booked $132 million in 340B savings. That is the system’s own number, on the system’s own page.
We just started a new series on 340B. Start here.
Federal law does not require 340B hospitals to pass any of those savings to patients at the pharmacy counter. Most do not. The Minnesota Department of Health published the only state-level 340B transparency report in the country, finding that Minnesota’s 340B hospitals took in $1.34 billion in net 340B revenue in 2024. The 12% largest covered entities captured more than 80% of that total. Hospitals’ 340B profits ran more than three times their uncompensated care spending.
There is no equivalent disclosure requirement in Missouri.
There is no public reporting of how much The University of Missouri Health’s $132 million in 340B savings reaches uninsured patients vs. how much funds general operations.
THE HIDDEN BILLION
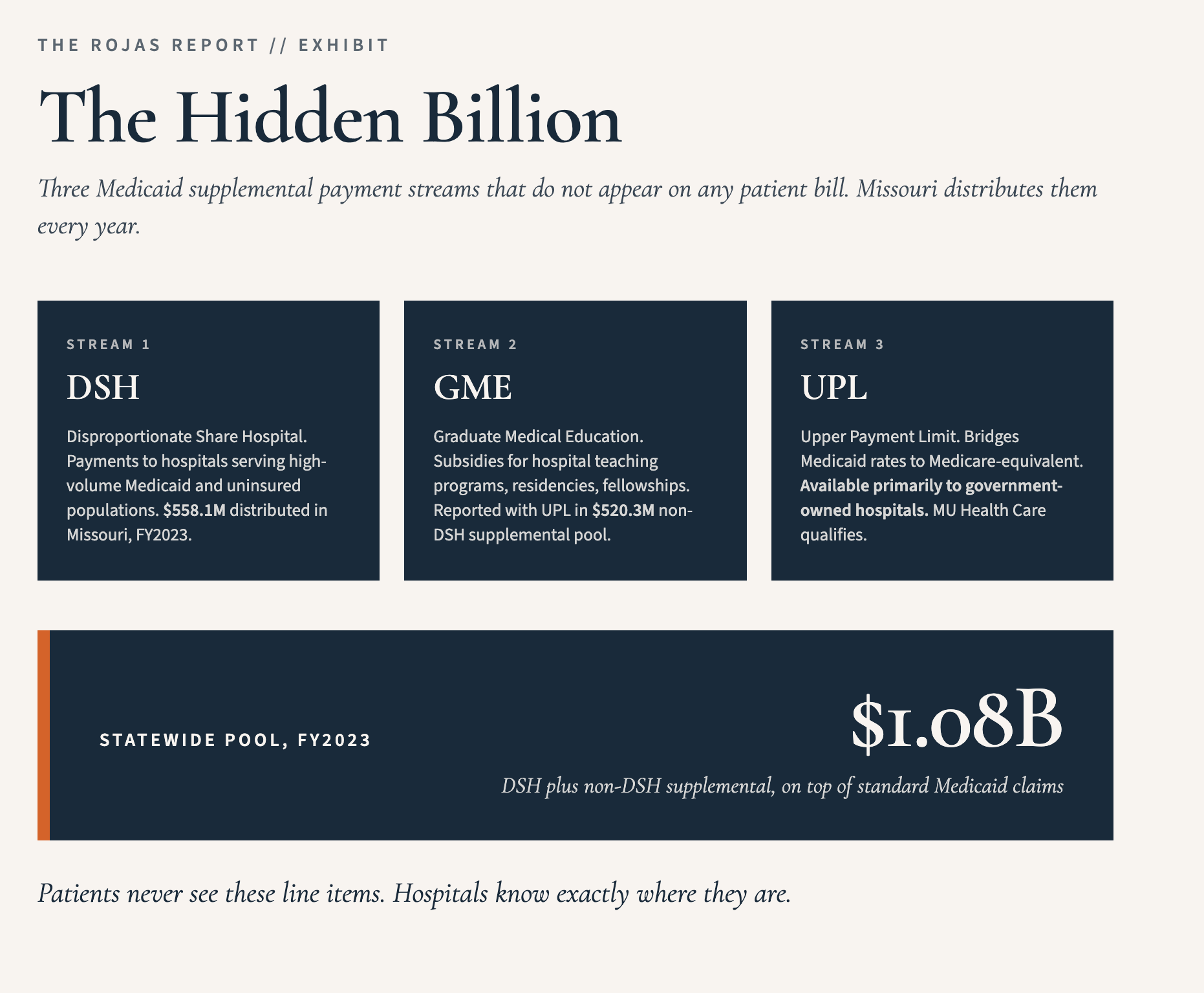
Beyond tax exemptions and 340B, The University of Missouri Health is a primary beneficiary of three Medicaid supplemental payment streams that almost no patient ever sees on a bill.
Disproportionate Share Hospital payments. Graduate Medical Education payments. Upper Payment Limit payments. These are state-administered, federally-matched programs that flow directly to hospitals serving Medicaid populations or operating teaching programs.
In FY2023, Missouri distributed $558.1 million in Medicaid DSH payments and $520.3 million in non-DSH supplemental payments (which includes UPL and GME) statewide. That is over $1 billion in supplemental Medicaid funding flowing to Missouri hospitals every year, on top of the standard Medicaid claims reimbursement they already receive.
UPL is restricted to government-owned hospitals. The University of Missouri Health is one of a small number of Missouri institutions eligible to receive it. The federal-state structure makes it a targeted subsidy for state-owned systems.
State of Missouri Rep. Jeff Knight and Sen. Kurtis Gregory filed the antitrust immunity bills in February. Most independent physicians in mid-Missouri learned of it from a guest commentary in April.
The deal gets made before the press release.
This newsletter is where you find out first.Join us! The Rojas Report
THE BILL
In February 2026, Rep. Jeff Knight, R-Lebanon, filed HB 3170. Sen. Kurtis Gregory, R-Marshall, filed the companion bill, SB 1602. Both bills do the same thing. Both grants the University of Missouri Health antitrust immunity to acquire any “hospital, medical or other health care facility” across a 25-county region in central Missouri.
The 25 counties are Adair, Audrain, Boone, Callaway, Camden, Chariton, Cole, Cooper, Gasconade, Howard, Linn, Macon, Maries, Miller, Moniteau, Monroe, Montgomery, Morgan, Osage, Pettis, Phelps, Pike, Pulaski, Randolph, and Saline.
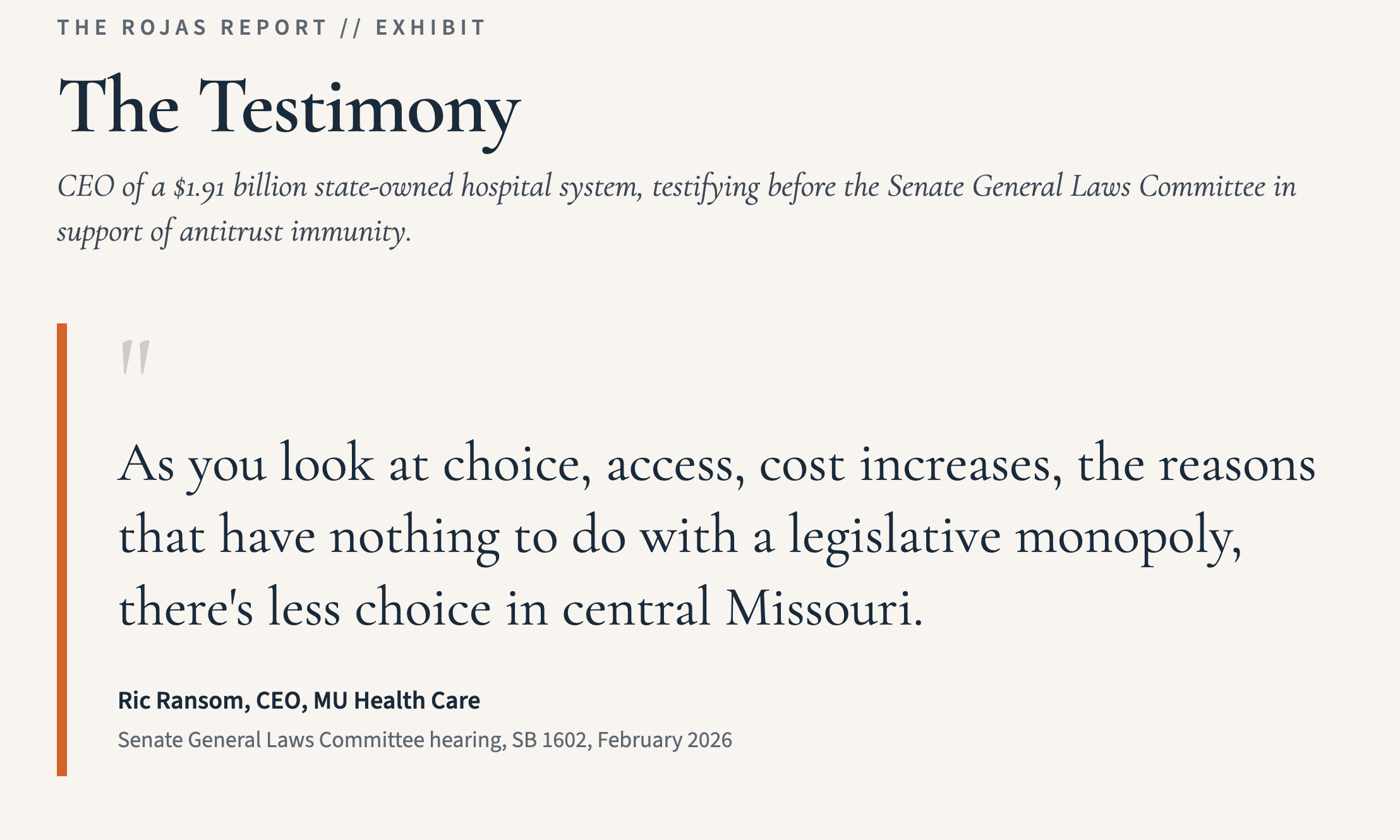
Ric Ransom personally testified in support before the Senate General Laws Committee. “As you look at choice, access, cost increases, the reasons that have nothing to do with a legislative monopoly, there’s less choice in central Missouri,” Ransom told the committee.
He is the CEO of a $1.9 billion state-owned hospital system, arguing before state senators that the way to address limited choice is to grant him legal immunity from antitrust review while he buys out the competition.
Kim Schlemeier, testifying in opposition, said the bill is more narrowly tailored than the 25-county frame suggests. “I believe that the legislation exempting them from antitrust is somewhat more narrowly tailored to Cole and Boone County, with the other 23 counties somewhat as window dressing.”
Boone is where The University of Missouri Health’s flagship University Hospital sits. Cole is where Capital Region Medical Center, recently absorbed, sits. Those are the two counties where The University of Missouri Health actually competes today. The other 23 counties are the stretch goal.
The closing line from opposition testimony lands as a direct hit on independent practice. “If this bill passes, specifically with its provisions for antitrust immunity, surgery centers in mid-Missouri would become entirely dependent upon the goodwill of a single entity, The University of Missouri Health, to keep their doors open.”
EVERY COUNTY THEY TOUCH PAYS TWICE
This is the closing argument and the reason this article exists.
Every hospital and independent medical practice that The University of Missouri Health acquires under HB 3170 or SB 1602 leaves the property tax rolls in the county where it sits. Permanently. The day after closing, that facility is state property. Boone County, Cole County, and every rural county named in the bill watches its assessable hospital tax base disappear, one acquisition at a time.
That tax base does not just vanish. It shifts. Every county budget has to be made whole. The shortfall comes out of every other property in the county: every farm, every house, every small business, every commercial parcel that is not state-owned. The bigger The University of Missouri gets, the heavier the property tax bill on every Missourian.
Why isn’t anyone calling this a tax bill?
It is a tax bill.
The bill was sold to legislators as the rescue plan for a rural hospital crisis. Sen. Gregory cited 20 hospital closures in Missouri over the past decade, ten of them rural. The Center for Healthcare Quality and Payment Reform reports that 50% of Missouri’s 58 remaining rural hospitals are at risk of closure, with 21% at immediate risk.
There is a rural hospital crisis.
The crisis is real.
That crisis is also solveable today without taxpayer help.
The bill is not a rescue.
It is a privatization of the cascade.
It transfers private hospital assets into a state instrumentality, removes them from local tax rolls, and shields the acquirer from antitrust review.
The diagnosis is clear:
Missouri’s rural hospitals are dying.
They are all fixable today.
The prognosis is what the lawmakers can talk the people of Missouri into next.
Independent physicians in 25 Missouri counties are about to compete against an antitrust-immune state monopoly.
No one in Jefferson City is coming to save them.
They are saving each other on this list. 100,000+ physicians and operators.
One signal.Read The Rojas Report
WHAT COMES NEXT FOR INDEPENDENT PRACTICE IN MID-MISSOURI
The 23 counties Schlemeier called “window dressing” are not actually window dressing. They are the option set. Every rural hospital in those counties that hits financial distress in the next 24 months is a potential acquisition target under the new framework. The bill does not just authorize specific deals. It builds the legal infrastructure for any future deal.
For independent surgery centers in Boone, Cole, Callaway, and Cooper counties, the practical effect of antitrust immunity is the removal of the only legal restraint that currently keeps payor contracting and physician hiring in something resembling balance. A monopoly with state-actor immunity has no antitrust ceiling. It has whatever the state legislature lets it have.
There is a captive insurance answer to part of this problem. There is a payor-contracting-aggregation answer to part of it. Neither of those answers exists anywhere in Missouri yet. They will. The question is whether the people who need them know they are coming before the next acquisition closes.
-Rojas out.
GLOSSARY
Section 115 IRC: Federal tax code provision that excludes from federal income tax any income a state derives from essential governmental functions. State universities and their hospital systems use it as the basis for federal tax exemption. Different from Section 501(c)(3), which governs nonprofits and requires Form 990 disclosure.
State instrumentality: A government entity operated by or as part of a state. The University of Missouri Health operates as part of the University of Missouri System and is treated as part of the state itself for tax purposes.
340B Drug Pricing Program: Federal program that requires drug manufacturers to provide discounted prices to “covered entities,” meaning hospitals serving disproportionate-share Medicaid populations and certain rural facilities. Hospitals dispense the discounted drugs at full reimbursement and book the spread as savings or revenue.
DSH (Disproportionate Share Hospital): Medicaid supplemental payments to hospitals that serve a disproportionate share of Medicaid and uninsured patients.
GME (Graduate Medical Education): Medicaid supplemental payments that subsidize hospital teaching programs, meaning residencies and fellowships.
UPL (Upper Payment Limit): Medicaid payments that bridge the gap between base Medicaid rates and what Medicare would have paid for the same services. Available primarily to government-owned hospitals.
Antitrust immunity: A legislative or regulatory exemption from antitrust enforcement. HB 3170 and SB 1602 grant MU Health Care immunity from federal and state antitrust laws for acquisitions in 25 counties.
Certificate of Need (CON): A state regulatory regime requiring healthcare providers to obtain government approval before opening new facilities, adding beds, or purchasing major equipment. Missouri maintains active CON laws.
Form 990: The annual return filed by 501(c)(3) tax-exempt organizations, including most nonprofit hospitals. Public document. Discloses revenue, executive compensation, and major contracts. State instrumentalities are not required to file it.
SOURCES
[1] Internal Revenue Code §115; University of Missouri System, “Notes to Financial Statements,” FY2025 Financial Report.
[2] University of Missouri Health Care, “Locations,” muhealth.org/about-us/locations.
[3] COMO Business Times, “Growing Healthcare into the Future,” January 2024.
[4] COMO Business Times, “Growing Healthcare into the Future,” January 2024 (Audrain County and Mexico clinic openings).
[5] University of Missouri System, “FY2025 Financial Report,” October 2025. [VERIFY: pull umsystem.edu PDF for exact FY2025 line items.]
[6] University of Missouri System, “Budget Facts FY 2026,” January 2026. [VERIFY: pull from umsystem.edu.]
[7] Show Me Mizzou, “University of Missouri Announces Ric Ransom as CEO of MU Health Care,” February 2023; Yahoo News, “Ric Ransom to lead University of Missouri Health Care,” February 2023.
[8] Public payroll records, 2024. [VERIFY: confirm exact figure via St. Louis Post-Dispatch Public Pay database (graphics.stltoday.com/apps/payrolls/salaries_2025/117) or Missouri Accountability Portal (mapyourtaxes.mo.gov).]
[9] University of Missouri Health Care, “Our 340B Story,” muhealth.org/about-us/340b.
[10] Lown Institute, “Hospital Fair Share Spending,” 2024 reports.
[11] Minnesota Department of Health, 340B Transparency Report, 2024 data published February 2026; STAT News, “Minnesota report shows large hospitals continue to dominate the 340B drug discount program,” February 2026.
[12] MACPAC, “Exhibit 24: Medicaid Supplemental Payments to Hospital Providers by State, FY 2023,” December 2024.
[13] Webster County Citizen, “Senate bill would allow MU Health Care to expand ownership in rural areas,” February 2026; KBIA, “Bill could broaden MU Health Care’s reach in rural counties,” February 20, 2026; Columbia Missourian, “Unprecedented legislation would allow MU Health Care to circumvent antitrust rules,” guest commentary; Missouri Independent, “Missouri’s rural hospital bill grants antitrust immunity without oversight,” April 6, 2026.
[14] Center for Healthcare Quality and Payment Reform, rural hospital closure risk analysis, cited in Missouri Independent, April 6, 2026.
My napkin math for our Lee Health was about what you report- 3% charity. That’s 7% below tithing.😎